

Exacerbation of primary intestinal lymphangiectasia during late pregnancy and recovery after delivery: A case report and literature review
- PMID: 28858117
- PMCID: PMC5585511
- DOI: 10.1097/MD.0000000000007928
Exacerbation of primary intestinal lymphangiectasia during late pregnancy and recovery after delivery: A case report and literature review
Abstract
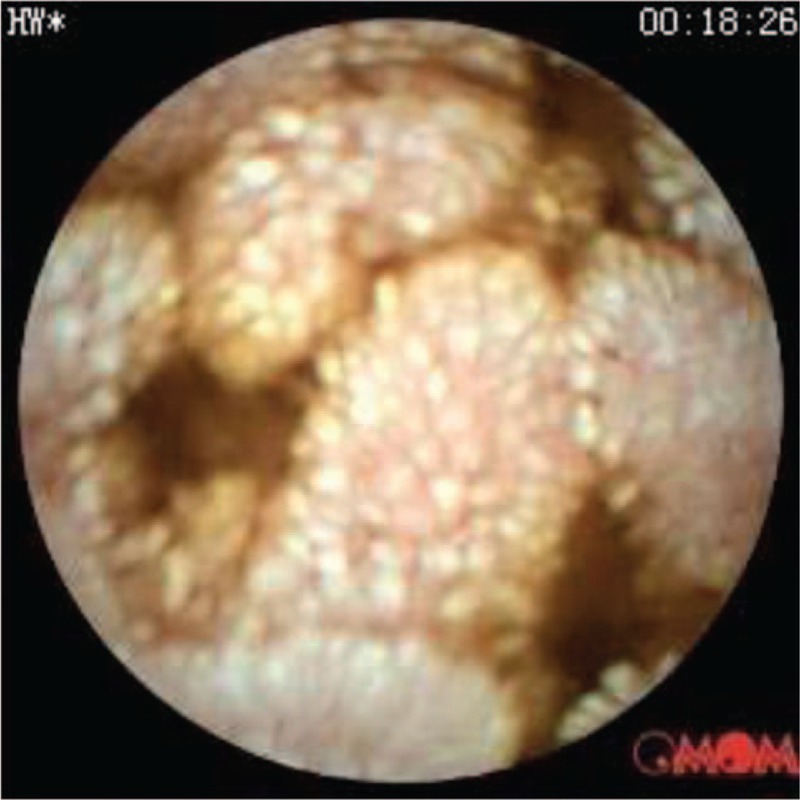
Rationale: Primary intestinal lymphangiectasia (PIL) is a rare disease characterized by dilated intestinal lacteals resulting in lymph leakage into the small bowel lumen. Main clinical features include intermittent diarrhea, hypoproteinemia. Scattered case reports suggested that PIL is compatible to pregnancy, but with increased complications.
Patient concerns: A 34-year-old woman with endoscopically diagnosed PIL presented to antenatal our clinic at 10 weeks into gestation. She reported strict adherence to low-fat/high-protein diet with medium-chain triglycerides (MCTs) supplementation. She was general well except for moderate edema and hypoalbuminemia. At 33 weeks, she developed diarrhea, nausea, and vomiting, with decreased fetal movements. One week later, she had an asthma attack. Nonstress test showed frequent variable deceleration.
Diagnoses: The diagnosis of PIL was established endoscopically 8 years earlier.
Interventions: Hypoalbuminemia was corrected with intravenous albumin administration. She also received corticosteroid therapy to promote fetal lung maturation in anticipation to early termination of the pregnancy.
Outcomes: A cesarean section was carried out at 34 weeks due to fetal distress. The baby girl was apparently healthy: weighing 2160 g, with an Apgar score of 9 at both 1 and 5 minutes. Symptoms dissipated rapidly after the delivery. The last follow-up visit at 15 months was unremarkable for both the mother and infant.
Lessons: PIL could be compatible with pregnancy, but requires strict adherence to dietary treatment, proper management of the symptoms (e.g., hypoalbuminemia), particularly during late gestation.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

References
-
- Waldmann TA, Steinfeld JL, Dutcher TF, et al. The role of gastrointestinal system in “Idiopathic hypoproteinemia”. Gastroenterology 1961;41:197–207. - PubMed
-
- Liu DT, Sherman AM. Case report—pregnancy and intestinal lymphangiectasis (familial neonatal hypoproteinaemia). Aust N Z J Obstet Gynaecol 1980;20:58–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
