

Natural History and Tumor Volume Kinetics of Papillary Thyroid Cancers During Active Surveillance
- PMID: 28859191
- PMCID: PMC5710258
- DOI: 10.1001/jamaoto.2017.1442
Natural History and Tumor Volume Kinetics of Papillary Thyroid Cancers During Active Surveillance
Abstract
Importance: Active surveillance of low-risk papillary thyroid cancer (PTC) is now an accepted alternative to immediate surgery, but experience with this approach outside of Japan is limited. The kinetics (probability, rate, and magnitude) of PTC tumor growth under active surveillance have not been well defined.
Objective: To describe the kinetics of PTC tumor growth during active surveillance.
Design, setting, and participants: Cohort study of 291 patients undergoing active surveillance for low-risk PTC (intrathyroidal tumors ≤1.5 cm) with serial tumor measurements via ultrasonography at a tertiary referral center in the United States.
Intervention: Active surveillance.
Main outcomes and measures: The cumulative incidence, rate, and magnitude of the change in tumor diameter or volume, as well as associations with patient and tumor characteristics.
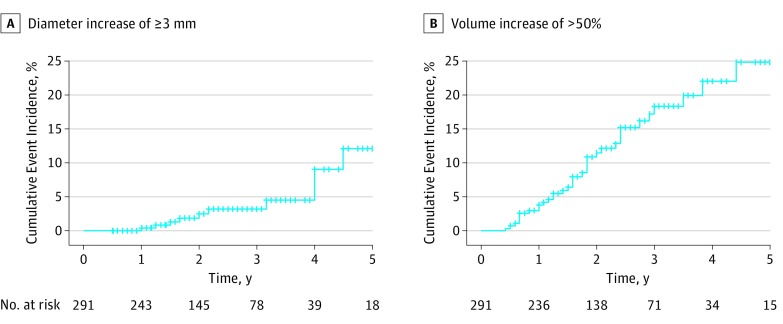
Results: Of the 291 patients, 219 (75.3%) were women; mean (SD) age was 52 (15) years. During a median (range) active surveillance of 25 (6-166) months, growth in tumor diameter of 3 mm or more was observed in 11 of 291 (3.8%) patients, with a cumulative incidence of 2.5% (2 years) and 12.1% (5 years). No regional or distant metastases developed during active surveillance. In all cases, 3-dimensional measurements of tumor volume allowed for earlier identification of growth (median, 8.2 months; range, 3-46 months before increase in tumor diameter). In multivariable analysis, both younger age at diagnosis (hazard ratio per year, 0.92; 95% CI, 0.87-0.98; P = .006) and risk category at presentation (hazard ratio for inappropriate, 55.17; 95% CI, 9.4-323.19; P < .001) were independently associated with the likelihood of tumor growth. Of the tumors experiencing volume growth, kinetics demonstrated a classic exponential growth pattern, with a median doubling time of 2.2 years (range, 0.5-4.8 years; median r2 = 0.75; range, 0.42-0.99).
Conclusions and relevance: The rates of tumor growth during active surveillance in a US cohort with PTCs measuring 1.5 cm or less were low. Serial measurement of tumor volumes may facilitate early identification of tumors that will continue to grow and thereby inform the timing of surveillance imaging and therapeutic interventions.
Conflict of interest statement
Figures


Comment in
-
Achieving Active Surveillance for Thyroid Cancer-Not a Euphemism for Watching a Ticking Time Bomb.JAMA Otolaryngol Head Neck Surg. 2017 Oct 1;143(10):1021-1022. doi: 10.1001/jamaoto.2017.1453. JAMA Otolaryngol Head Neck Surg. 2017. PMID: 28859186 No abstract available.
-
Expanding the Options for Patient-Guided Decision Making in Papillary Thyroid Cancer.JAMA. 2018 Jan 2;319(1):76-77. doi: 10.1001/jama.2017.18608. JAMA. 2018. PMID: 29297064 No abstract available.
References
-
- Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014;140(4):317-322. - PubMed
-
- Davies L, Ouellette M, Hunter M, Welch HG. The increasing incidence of small thyroid cancers: where are the cases coming from? Laryngoscope. 2010;120(12):2446-2451. - PubMed
-
- Vaccarella S, Franceschi S, Bray F, Wild CP, Plummer M, Dal Maso L. Worldwide thyroid-cancer epidemic? the increasing impact of overdiagnosis. N Engl J Med. 2016;375(7):614-617. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
