

Measurement of Intraocular Pressure by Patients With Glaucoma
- PMID: 28859192
- PMCID: PMC5710491
- DOI: 10.1001/jamaophthalmol.2017.3151
Measurement of Intraocular Pressure by Patients With Glaucoma
Abstract
Importance: The ability of patients to measure their own intraocular pressure (IOP) would allow more frequent measurements and better appreciation of peak IOP and IOP fluctuation.
Objective: To examine whether patients with glaucoma can perform self-tonometry using a rebound tonometer and examine patient acceptability.
Design, setting, and participants: An observational study in which IOP was assessed using Goldmann applanation tonometry and a rebound tonometer. Consecutive patients were provided with a patient information sheet and those consenting to take part in the study received standardized self-tonometry training and were then instructed to measure their own IOP under observation. This study was conducted at a glaucoma clinic at a university hospital from March 1, 2016, to December 30, 2016, and included both eyes of 100 patients with glaucoma or ocular hypertension.
Main outcomes and measures: The percentage of patients who could successfully perform self-tonometry. Complete success was defined by a good technique and an IOP reading within 5 mm Hg of that obtained by a clinician using the same device. A 3-item questionnaire was used to examine perceptions of self-tonometry among patients.
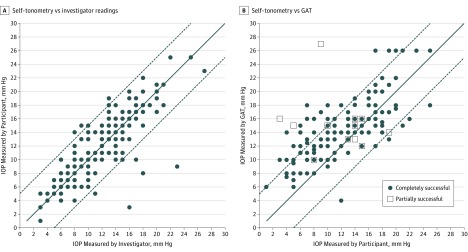
Results: Among the 100 patients, the mean (SD) age was 67.5 (10.9) years (53% female). A total 73 of 100 patients (73%) met the complete success criteria. An additional 6 patients could use the device but had IOP readings greater than 5 mm Hg different from those obtained by the clinician. On average, IOP by the rebound tonometer was 2.66 mm Hg lower than Goldmann applanation tonometry (95% limits of agreement, -3.48 to 8.80 mm Hg). The IOPs with the rebound tonometer were similar whether obtained by self-tonometry or investigator, with excellent reproducibility with an intraclass correlation coefficient of 0.903 (95% CI, 0.867-0.928). A total of 56 of 79 successful or partially successful patients (71%) felt self-tonometry was easy, with 73 of 79 (92%) reporting self-tonometry to be comfortable, and a similar number happy to perform self-tonometry in the future.
Conclusions and relevance: Most patients could perform self-tonometry and the method was acceptable to patients. Self-tonometry has the potential to improve patient engagement, while also providing a more complete picture of IOP changes over time.
Conflict of interest statement
Figures
Comment in
-
Home Tonometry-Can We? Should We?JAMA Ophthalmol. 2017 Oct 1;135(10):1036. doi: 10.1001/jamaophthalmol.2017.3194. JAMA Ophthalmol. 2017. PMID: 28859198 No abstract available.
References
-
- Sit AJ. Intraocular pressure variations: causes and clinical significance. Can J Ophthalmol. 2014;49(6):484-488. - PubMed
-
- Bliziotis IA, Destounis A, Stergiou GS. Home versus ambulatory and office blood pressure in predicting target organ damage in hypertension: a systematic review and meta-analysis. J Hypertens. 2012;30(7):1289-1299. - PubMed
-
- Sakamoto M, Kanamori A, Fujihara M, Yamada Y, Nakamura M, Negi A. Assessment of IcareONE rebound tonometer for self-measuring intraocular pressure. Acta Ophthalmol. 2014;92(3):243-248. - PubMed
-
- Rosentreter A, Jablonski KS, Mellein AC, Gaki S, Hueber A, Dietlein TS. A new rebound tonometer for home monitoring of intraocular pressure. Graefes Arch Clin Exp Ophthalmol. 2011;249(11):1713-1719. - PubMed
-
- Moreno-Montañés J, Martínez-de-la-Casa JM, Sabater AL, Morales-Fernandez L, Sáenz C, Garcia-Feijoo J. Clinical evaluation of the new rebound tonometers Icare PRO and Icare ONE compared with the Goldmann tonometer. J Glaucoma. 2015;24(7):527-532. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
