

Decision aids for second-line palliative chemotherapy: a randomised phase II multicentre trial
- PMID: 28859646
- PMCID: PMC5580234
- DOI: 10.1186/s12911-017-0529-y
Decision aids for second-line palliative chemotherapy: a randomised phase II multicentre trial
Abstract
Background: There is increasing recognition of the delicate balance between the modest benefits of palliative chemotherapy and the burden of treatment. Decision aids (DAs) can potentially help patients with advanced cancer with these difficult treatment decisions, but providing detailed information could have an adverse impact on patients' well-being. The objective of this randomised phase II study was to evaluate the safety and efficacy of DAs for patients with advanced cancer considering second-line chemotherapy.
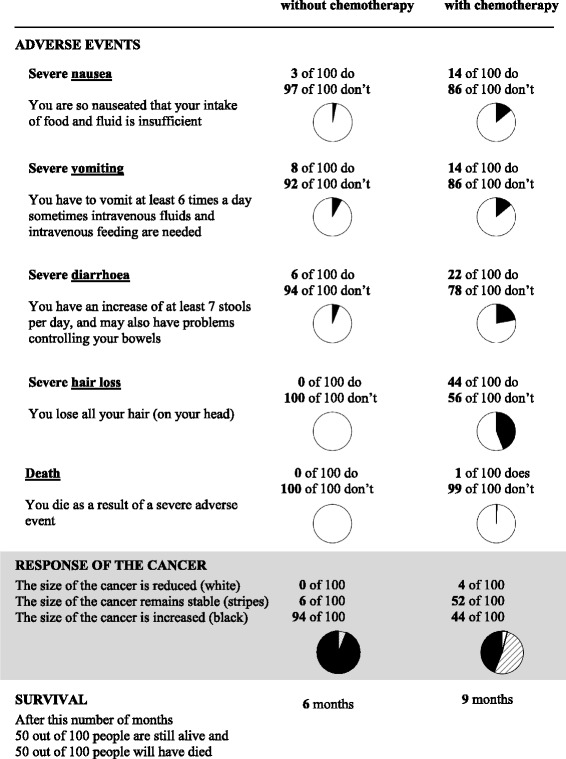
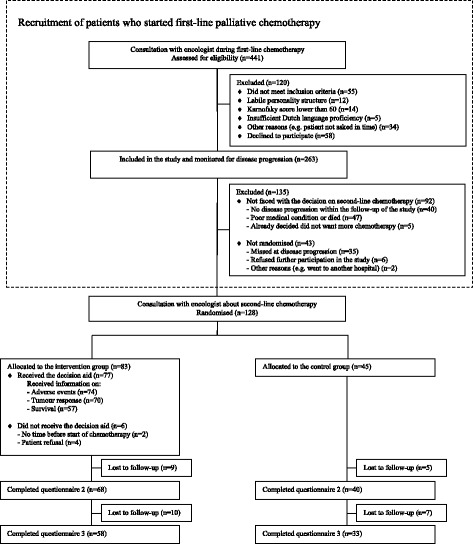
Methods: Patients with advanced breast or colorectal cancer considering second-line treatment were randomly assigned to usual care (control group) or usual care plus a DA (intervention group) in a 1:2 ratio. A nurse offered a DA with information on adverse events, tumour response and survival. Outcome measures included patient-reported well-being (primary outcome: anxiety) and quality of the decision-making process and the resulting choice.
Results: Of 128 patients randomised, 45 were assigned to the control group and 83 to the intervention group. Median age was 62 years (range 32-81), 63% were female, and 73% had colorectal cancer. The large majority of patients preferred treatment with chemotherapy (87%) and subsequently commenced treatment with chemotherapy (86%). No adverse impact on patients' well-being was found and nurses reported that consultations in which the DAs were offered went well. Being offered the DA was associated with stronger treatment preferences (3.0 vs. 2.5; p=0.030) and increased subjective knowledge (6.7 vs. 6.3; p=0.022). Objective knowledge, risk perception and perceived involvement were comparable between the groups.
Conclusions: DAs containing detailed risk information on second-line palliative treatment could be delivered to patients with advanced cancer without having an adverse impact on patient well-being. Surprisingly, the DAs only marginally improved the quality of the decision-making process. The effectiveness of DAs for palliative treatment decisions needs further exploration.
Trial registration: Netherlands Trial Registry (NTR): NTR1113 (registered on 2 November 2007).
Keywords: Breast cancer; Colorectal cancer; Decision aids; Oncology; Palliative chemotherapy; Second-line.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was obtained from the regional ethics review committee (CMO Arnhem-Nijmegen) as well as the research ethics committees of all participating hospitals. All patients included in the study provided written informed consent. Obtaining informed consent from health professionals was not required according to local regulations.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Peppercorn JM, Smith TJ, Helft PR, Debono DJ, Berry SR, Wollins DS, Hayes DM, Von Roenn JH, Schnipper LE. American Society of Clinical O. American society of clinical oncology statement: toward individualized care for patients with advanced cancer. J Clin Oncol. 2011;29(6):755–760. doi: 10.1200/JCO.2010.33.1744. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
