

Dysglycemia and Index60 as Prediagnostic End Points for Type 1 Diabetes Prevention Trials
- PMID: 28860125
- PMCID: PMC5652585
- DOI: 10.2337/dc17-0916
Dysglycemia and Index60 as Prediagnostic End Points for Type 1 Diabetes Prevention Trials
Abstract
Objective: We assessed dysglycemia and a T1D Diagnostic Index60 (Index60) ≥1.00 (on the basis of fasting C-peptide, 60-min glucose, and 60-min C-peptide levels) as prediagnostic end points for type 1 diabetes among Type 1 Diabetes TrialNet Pathway to Prevention Study participants.
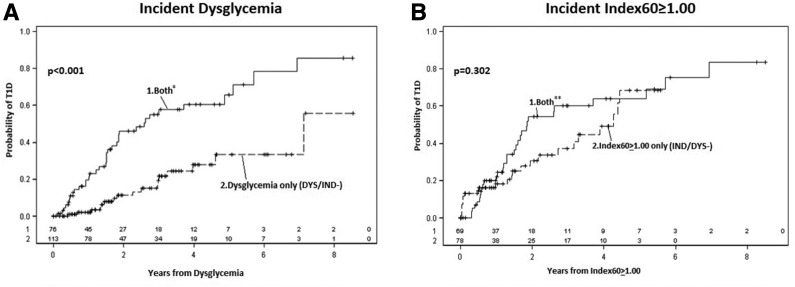
Research design and methods: Two cohorts were analyzed: 1) baseline normoglycemic oral glucose tolerance tests (OGTTs) with an incident dysglycemic OGTT and 2) baseline Index60 <1.00 OGTTs with an incident Index60 ≥1.00 OGTT. Incident dysglycemic OGTTs were divided into those with (DYS/IND+) and without (DYS/IND-) concomitant Index60 ≥1.00. Incident Index60 ≥1.00 OGTTs were divided into those with (IND/DYS+) and without (IND/DYS-) concomitant dysglycemia.
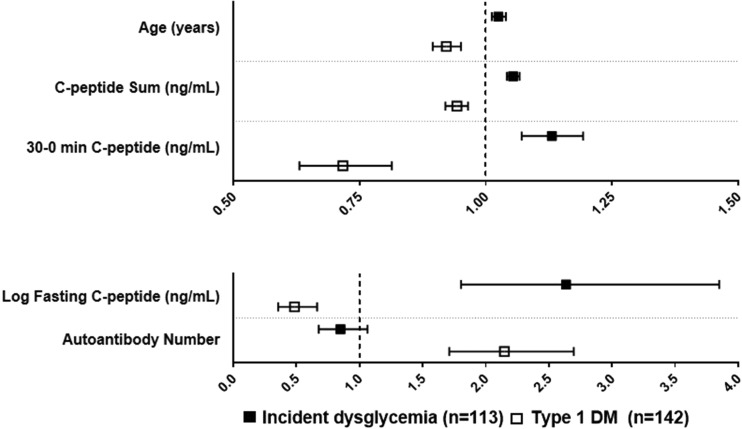
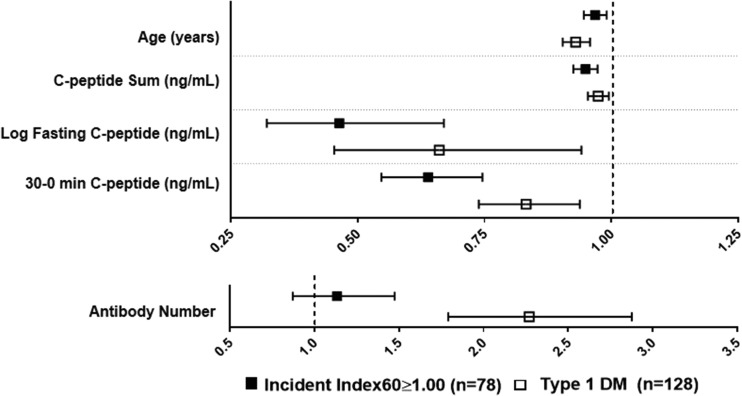
Results: The cumulative incidence for type 1 diabetes was greater after IND/DYS- than after DYS/IND- (P < 0.01). Within the normoglycemic cohort, the cumulative incidence of type 1 diabetes was higher after DYS/IND+ than after DYS/IND- (P < 0.001), whereas within the Index60 <1.00 cohort, the cumulative incidence after IND/DYS+ and after IND/DYS- did not differ significantly. Among nonprogressors, type 1 diabetes risk at the last OGTT was greater for IND/DYS- than for DYS/IND- (P < 0.001). Hazard ratios (HRs) of DYS/IND- with age and 30- to 0-min C-peptide were positive (P < 0.001 for both), whereas HRs of type 1 diabetes with these variables were inverse (P < 0.001 for both). In contrast, HRs of IND/DYS- and type 1 diabetes with age and 30- to 0-min C-peptide were consistent (all inverse [P < 0.01 for all]).
Conclusions: The findings suggest that incident dysglycemia without Index60 ≥1.00 is a suboptimal prediagnostic end point for type 1 diabetes. Measures that include both glucose and C-peptide levels, such as Index60 ≥1.00, appear better suited as prediagnostic end points.
© 2017 by the American Diabetes Association.
Figures
References
-
- Eisenbarth GS. Type I diabetes mellitus. A chronic autoimmune disease. N Engl J Med 1986;314:1360–1368 - PubMed
-
- Gorsuch AN, Spencer KM, Lister J, et al. Evidence for a long prediabetic period in type I (insulin-dependent) diabetes mellitus. Lancet 1981;2:1363–1365 - PubMed
-
- Sosenko JM, Palmer JP, Greenbaum CJ, et al. Patterns of metabolic progression to type 1 diabetes in the Diabetes Prevention Trial–Type 1. Diabetes Care 2006;29:643–649 - PubMed
MeSH terms
Substances
Grants and funding
- UC4 DK106993/DK/NIDDK NIH HHS/United States
- U01 DK085461/DK/NIDDK NIH HHS/United States
- R01 DK093954/DK/NIDDK NIH HHS/United States
- U01 DK106994/DK/NIDDK NIH HHS/United States
- U01 DK085453/DK/NIDDK NIH HHS/United States
- U01 DK107014/DK/NIDDK NIH HHS/United States
- I01 BX001733/BX/BLRD VA/United States
- U01 DK085504/DK/NIDDK NIH HHS/United States
- U01 DK085466/DK/NIDDK NIH HHS/United States
- U01 DK085465/DK/NIDDK NIH HHS/United States
- U01 DK085499/DK/NIDDK NIH HHS/United States
- U01 DK061010/DK/NIDDK NIH HHS/United States
- U01 DK085509/DK/NIDDK NIH HHS/United States
- U01 DK103153/DK/NIDDK NIH HHS/United States
- U01 DK061042/DK/NIDDK NIH HHS/United States
- U01 DK103180/DK/NIDDK NIH HHS/United States
- U01 DK103282/DK/NIDDK NIH HHS/United States
- U01 DK103266/DK/NIDDK NIH HHS/United States
- U01 DK085476/DK/NIDDK NIH HHS/United States
- U01 DK061058/DK/NIDDK NIH HHS/United States
- U01 DK106984/DK/NIDDK NIH HHS/United States
- U01 DK061034/DK/NIDDK NIH HHS/United States
- U01 DK107013/DK/NIDDK NIH HHS/United States
- P30 DK097512/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
