

Opioid Receptor Activation Impairs Hypoglycemic Counterregulation in Humans
- PMID: 28860128
- PMCID: PMC5652610
- DOI: 10.2337/db16-1478
Opioid Receptor Activation Impairs Hypoglycemic Counterregulation in Humans
Abstract
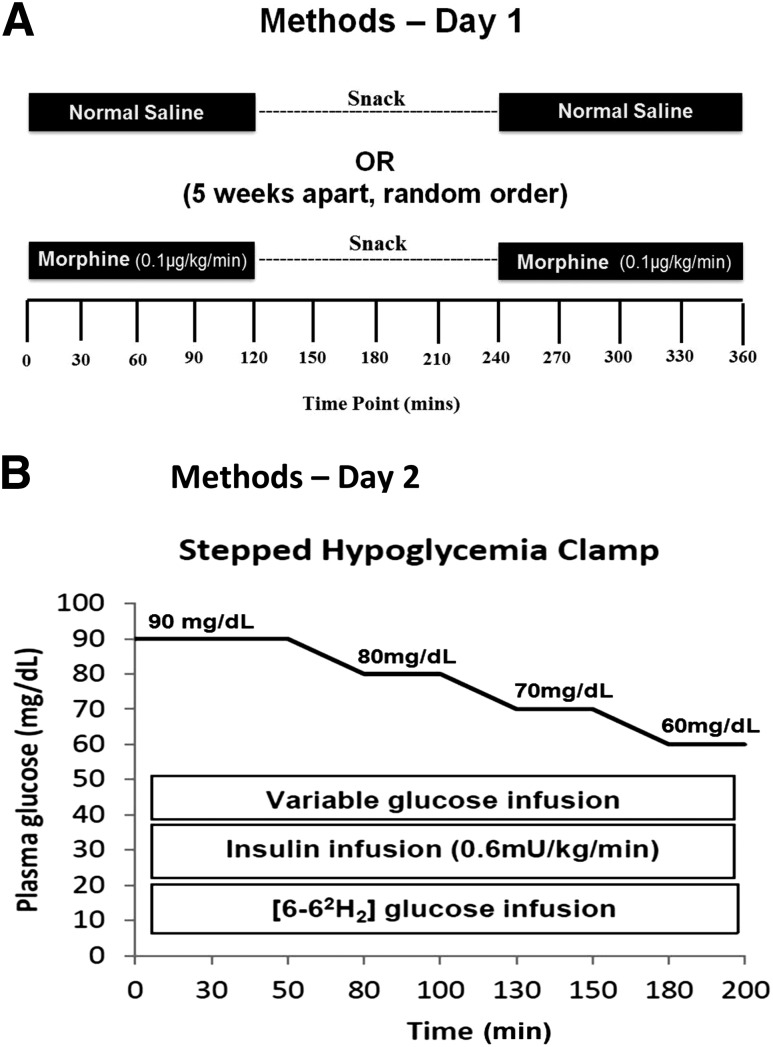
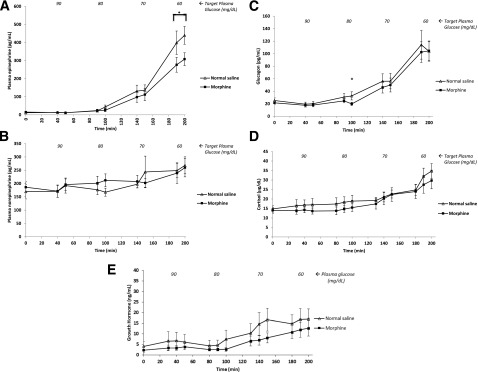
Although intensive glycemic control improves outcomes in type 1 diabetes mellitus (T1DM), iatrogenic hypoglycemia limits its attainment. Recurrent and/or antecedent hypoglycemia causes blunting of protective counterregulatory responses, known as hypoglycemia-associated autonomic failure (HAAF). To determine whether and how opioid receptor activation induces HAAF in humans, 12 healthy subjects without diabetes (7 men, age 32.3 ± 2.2 years, BMI 25.1 ± 1.0 kg/m2) participated in two study protocols in random order over two consecutive days. On day 1, subjects received two 120-min infusions of either saline or morphine (0.1 μg/kg/min), separated by a 120-min break (all euglycemic). On day 2, subjects underwent stepped hypoglycemic clamps (nadir 60 mg/dL) with evaluation of counterregulatory hormonal responses, endogenous glucose production (EGP, using 6,6-D2-glucose), and hypoglycemic symptoms. Morphine induced an ∼30% reduction in plasma epinephrine response together with reduced EGP and hypoglycemia-associated symptoms on day 2. Therefore, we report the first studies in humans demonstrating that pharmacologic opioid receptor activation induces some of the clinical and biochemical features of HAAF, thus elucidating the individual roles of various receptors involved in HAAF's development and suggesting novel pharmacologic approaches for safer intensive glycemic control in T1DM.
Trial registration: ClinicalTrials.gov NCT00678145.
© 2017 by the American Diabetes Association.
Figures




References
-
- The DCCT Research Group Epidemiology of severe hypoglycemia in the diabetes control and complications trial. Am J Med 1991;90:450–459 - PubMed
-
- Group UKHS; UK Hypoglycaemia Study Group . Risk of hypoglycaemia in types 1 and 2 diabetes: effects of treatment modalities and their duration. Diabetologia 2007;50:1140–1147 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
