

Creatine ( methyl-d3) dilution in urine for estimation of total body skeletal muscle mass: accuracy and variability vs. MRI and DXA
- PMID: 28860169
- PMCID: PMC6048459
- DOI: 10.1152/japplphysiol.00455.2016
Creatine ( methyl-d3) dilution in urine for estimation of total body skeletal muscle mass: accuracy and variability vs. MRI and DXA
Abstract
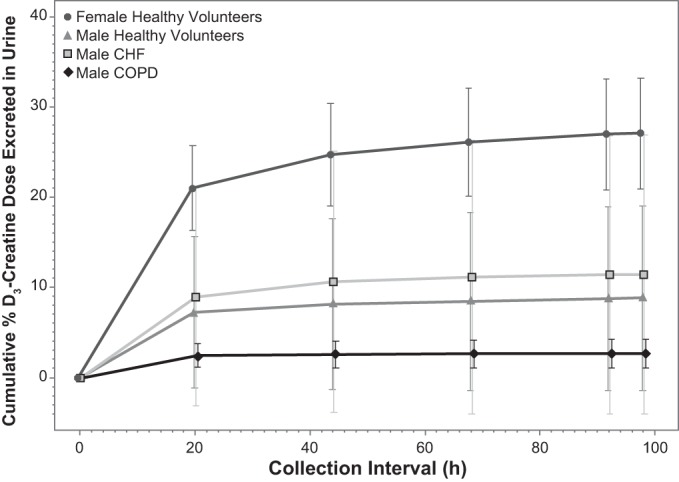
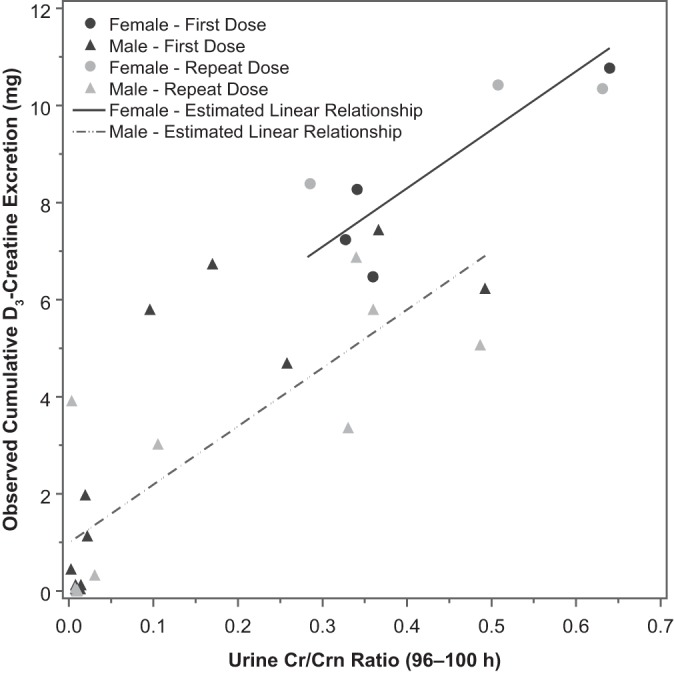
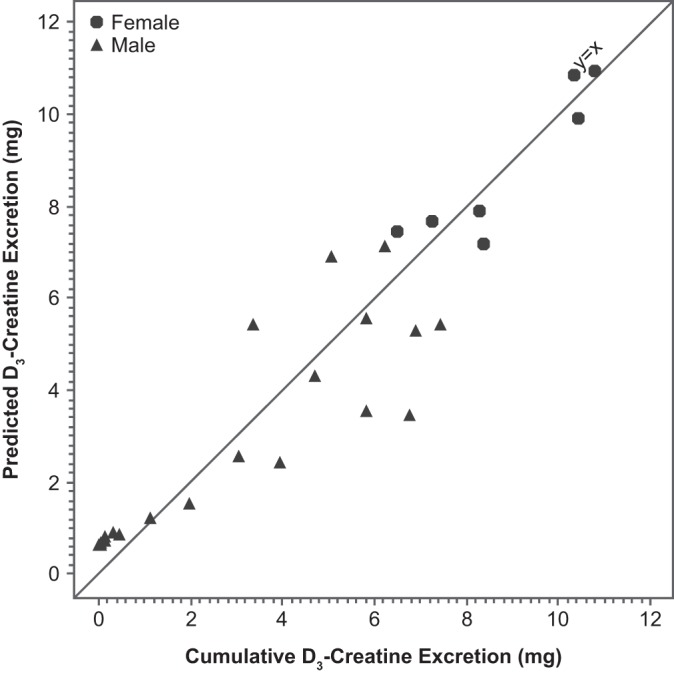
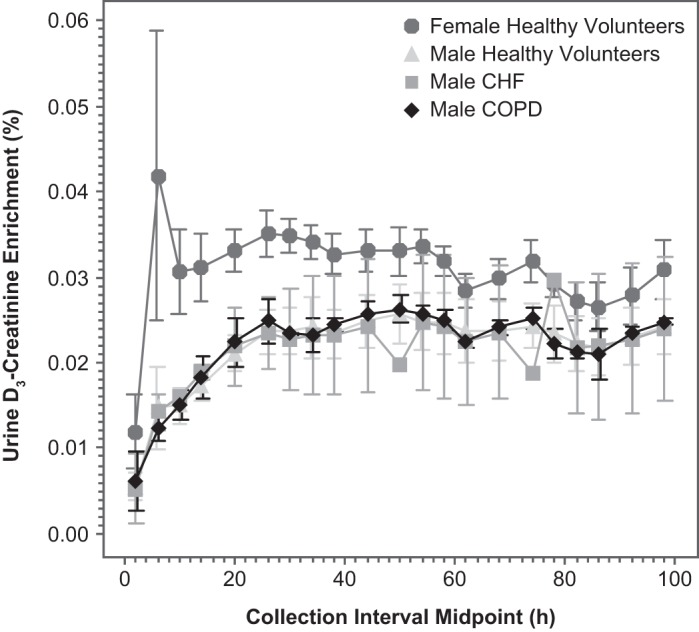
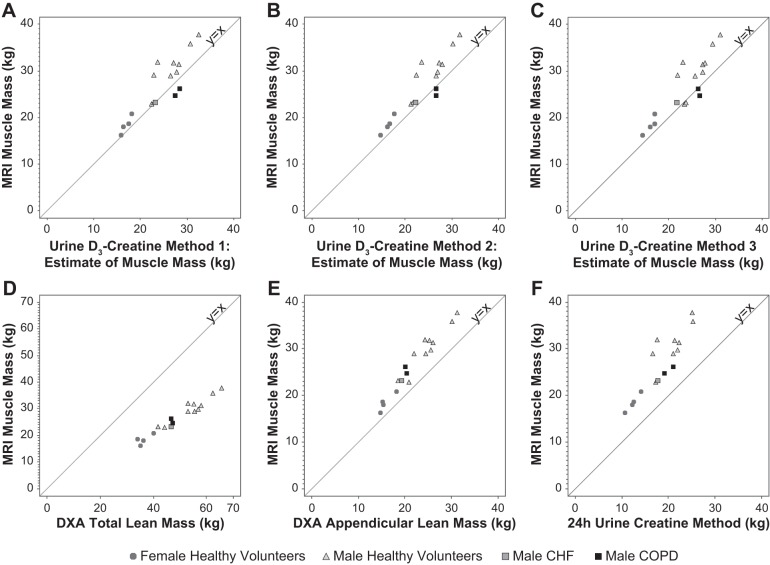
A noninvasive method to estimate muscle mass based on creatine ( methyl-d3) (D3-creatine) dilution using fasting morning urine was evaluated for accuracy and variability over a 3- to 4-mo period. Healthy older (67- to 80-yr-old) subjects ( n = 14) with muscle wasting secondary to aging and four patients with chronic disease (58-76 yr old) fasted overnight and then received an oral 30-mg dose of D3-creatine at 8 AM ( day 1). Urine was collected during 4 h of continued fasting and then at consecutive 4- to 8-h intervals through day 5. Assessment was repeated 3-4 mo later in 13 healthy subjects and 1 patient with congestive heart failure. Deuterated and unlabeled creatine and creatinine were measured using liquid chromatography-tandem mass spectrometry. Total body creatine pool size and muscle mass were calculated from D3-creatinine enrichment in urine. Muscle mass was also measured by whole body MRI and 24-h urine creatinine, and lean body mass (LBM) was measured by dual-energy X-ray absorptiometry (DXA). D3-creatinine urinary enrichment from day 5 provided muscle mass estimates that correlated with MRI for all subjects ( r = 0.88, P < 0.0001), with less bias [difference from MRI = -3.00 ± 2.75 (SD) kg] than total LBM assessment by DXA, which overestimated muscle mass vs. MRI (+22.5 ± 3.7 kg). However, intraindividual variability was high with the D3-creatine dilution method, with intrasubject SD for estimated muscle mass of 2.5 kg vs. MRI (0.5 kg) and DXA (0.8 kg). This study supports further clinical validation of the D3-creatine method for estimating muscle mass. NEW & NOTEWORTHY Measurement of creatine ( methyl-d3) (D3-creatine) and D3-creatinine excretion in fasted morning urine samples may be a simple, less costly alternative to MRI or dual-energy X-ray absorptiometry (DXA) to calculate total body muscle mass. The D3-creatine enrichment method provides estimates of muscle mass that correlate well with MRI, and with less bias than DXA. However, intraindividual variability is high with the D3-creatine method. Studies to refine the spot urine sample method for estimation of muscle mass may be warranted.
Keywords: creatine; creatinine; dual-energy X-ray absorptiometry; lean mass; muscle mass.
Figures
References
-
- Baracos V, Caserotti P, Earthman CP, Fields D, Gallagher D, Hall KD, Heymsfield SB, Müller MJ, Rosen AN, Pichard C, Redman LM, Shen W, Shepherd JA, Thomas D. Advances in the science and application of body composition measurement. JPEN J Parenter Enteral Nutr 36: 96–107, 2012. doi: 10.1177/0148607111417448. - DOI - PMC - PubMed
-
- Bianchi L, Ferrucci L, Cherubini A, Maggio M, Bandinelli S, Savino E, Brombo G, Zuliani G, Guralnik JM, Landi F, Volpato S. The predictive value of the EWGSOP definition of sarcopenia: results from the InCHIANTI study. J Gerontol A Biol Sci Med Sci 71: 259–264, 2016. doi: 10.1093/gerona/glv129. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases