

Differences in characteristics of glucose intolerance between patients with NAFLD and chronic hepatitis C as determined by CGMS
- PMID: 28860506
- PMCID: PMC5579047
- DOI: 10.1038/s41598-017-09256-4
Differences in characteristics of glucose intolerance between patients with NAFLD and chronic hepatitis C as determined by CGMS
Abstract
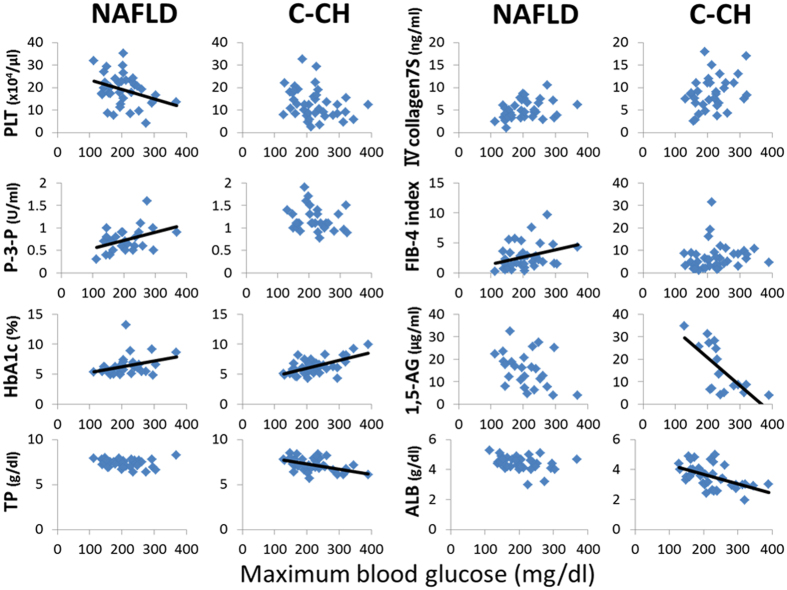
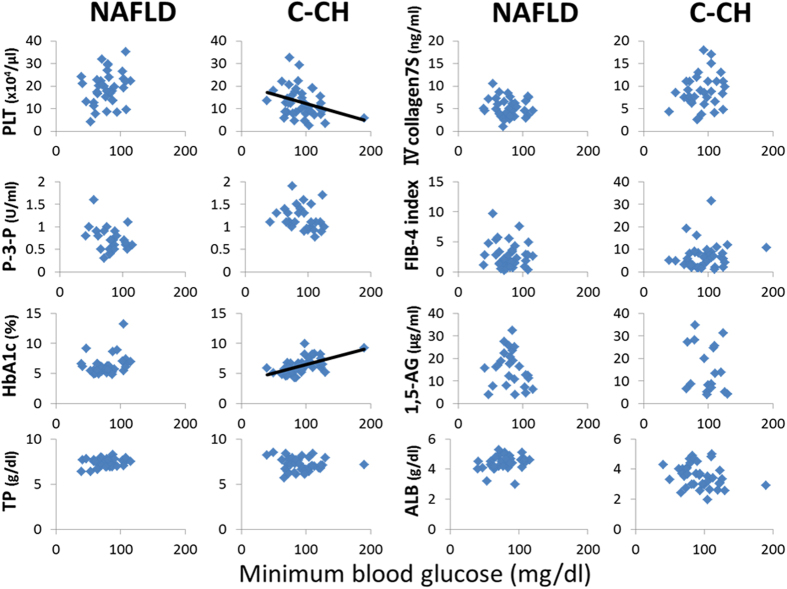
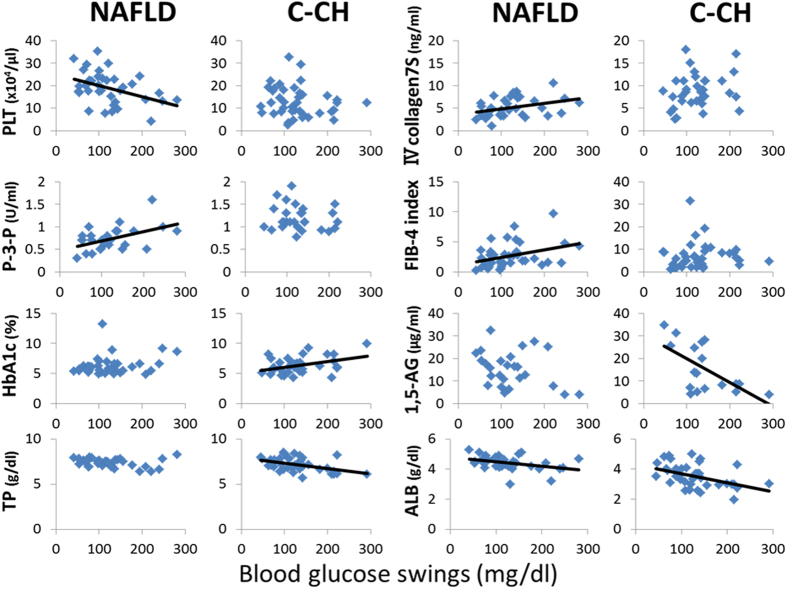
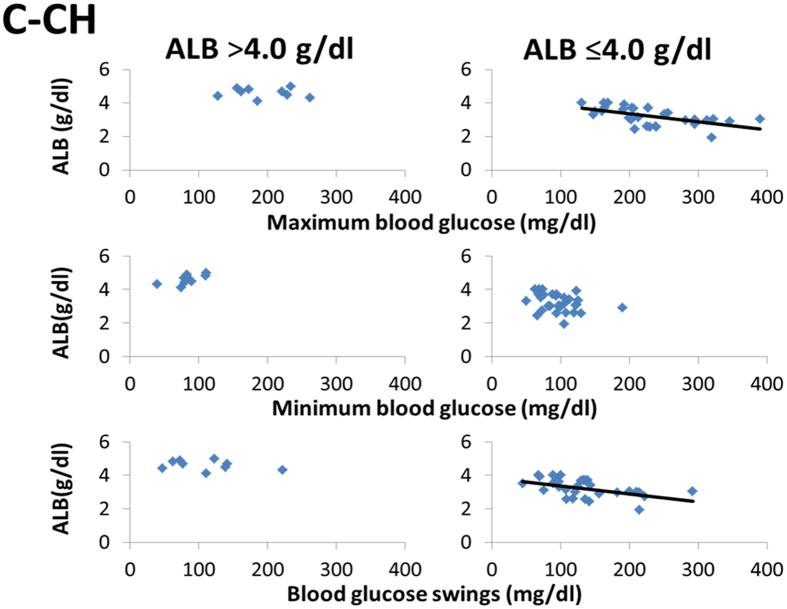
Glucose intolerance frequently develops in accordance with the progression of chronic liver disease. However, differences in the characteristics of glucose intolerance between patients with nonalcoholic fatty liver disease (NAFLD) and those with chronic hepatitis C (C-CH) remain incompletely understood. To clarify these differences, patients with NAFLD (n = 37) and C-CH (n = 40) were evaluated with a continuous glucose monitoring system (CGMS). In the patients with NAFLD, Maximum blood glucose concentration and blood glucose swings were significantly correlated with hepatic fibrosis markers. In the patients with C-CH, however, those two CGMS parameters were negatively correlated with the serum albumin (ALB) concentration. Furthermore, in the patients with C-CH with an ALB concentration of ≤4.0 g/dl, those two CGMS parameters were negatively correlated with the ALB concentration with greater statistical significance. In conclusion, obvious differences in the characteristics of glucose intolerance between patients with NAFLD and those with C-CH were clarified. In patients with NAFLD, glucose intolerance gradually progressed in accordance with the progression of hepatic fibrosis. In those with C-CH, glucose intolerance suddenly developed upon the appearance of hypoalbuminaemia.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
