

Radiomics strategies for risk assessment of tumour failure in head-and-neck cancer
- PMID: 28860628
- PMCID: PMC5579274
- DOI: 10.1038/s41598-017-10371-5
Radiomics strategies for risk assessment of tumour failure in head-and-neck cancer
Abstract
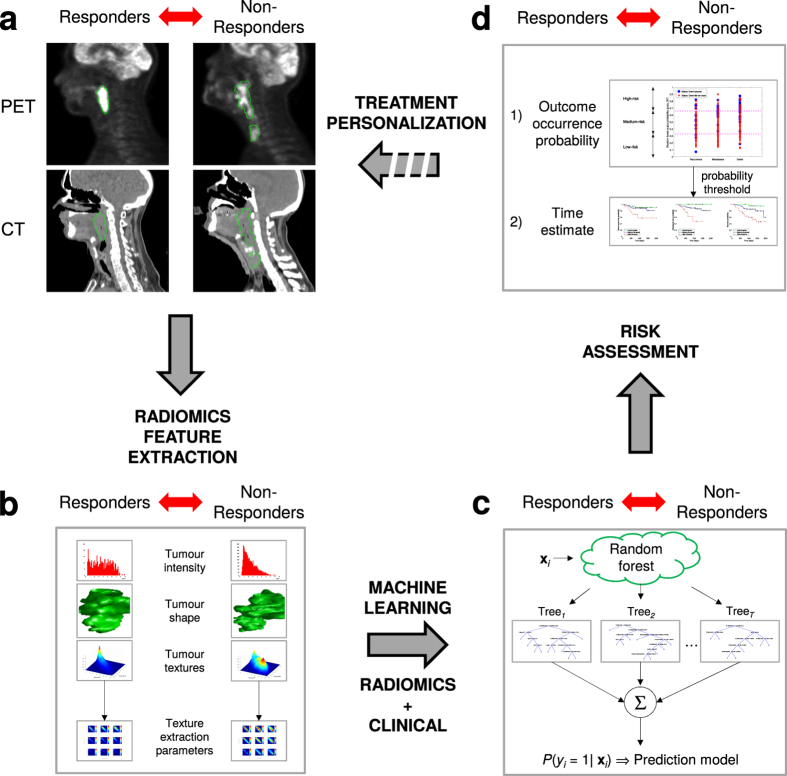
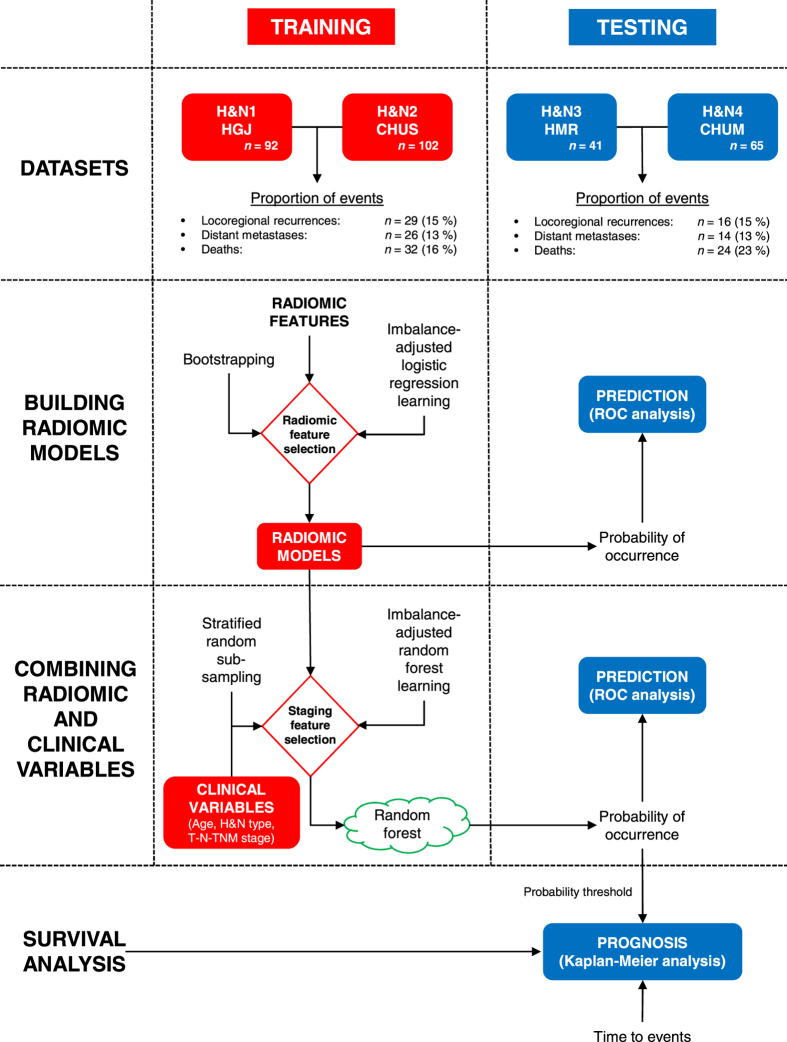
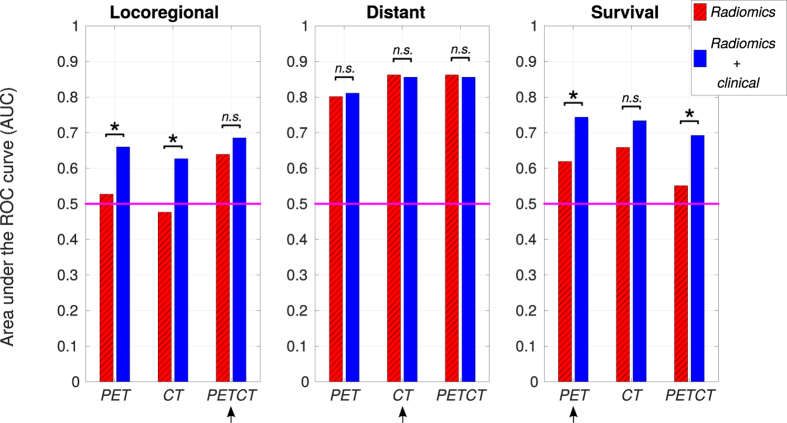
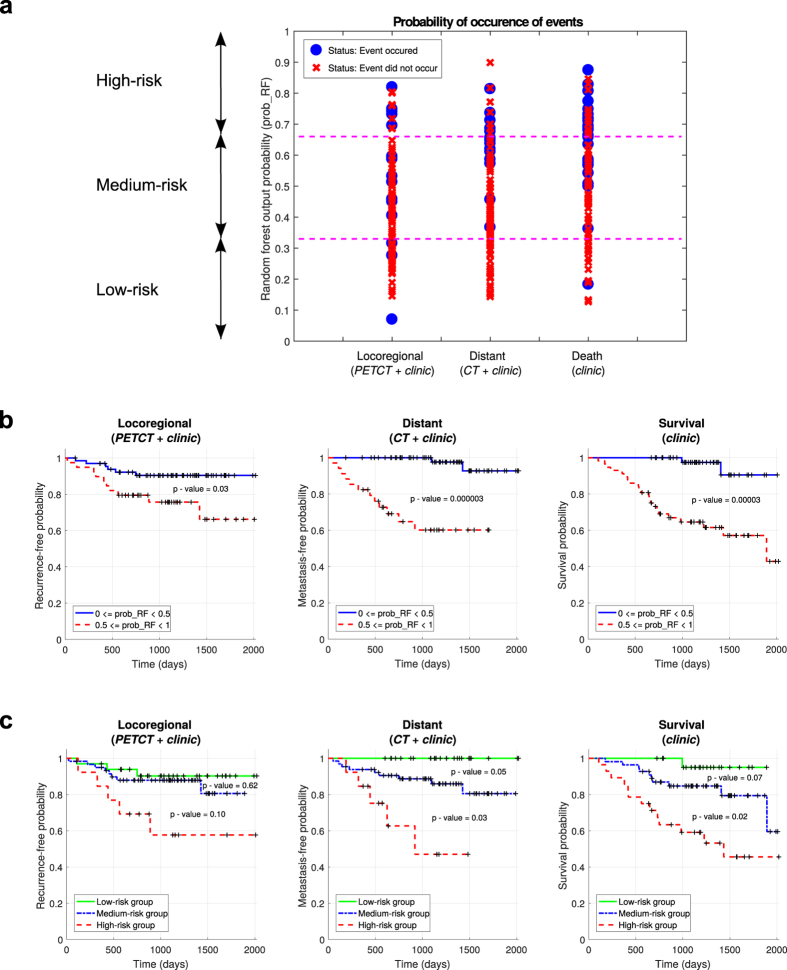
Quantitative extraction of high-dimensional mineable data from medical images is a process known as radiomics. Radiomics is foreseen as an essential prognostic tool for cancer risk assessment and the quantification of intratumoural heterogeneity. In this work, 1615 radiomic features (quantifying tumour image intensity, shape, texture) extracted from pre-treatment FDG-PET and CT images of 300 patients from four different cohorts were analyzed for the risk assessment of locoregional recurrences (LR) and distant metastases (DM) in head-and-neck cancer. Prediction models combining radiomic and clinical variables were constructed via random forests and imbalance-adjustment strategies using two of the four cohorts. Independent validation of the prediction and prognostic performance of the models was carried out on the other two cohorts (LR: AUC = 0.69 and CI = 0.67; DM: AUC = 0.86 and CI = 0.88). Furthermore, the results obtained via Kaplan-Meier analysis demonstrated the potential of radiomics for assessing the risk of specific tumour outcomes using multiple stratification groups. This could have important clinical impact, notably by allowing for a better personalization of chemo-radiation treatments for head-and-neck cancer patients from different risk groups.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Lambin P, et al. Rapid Learning health care in oncology – an approach towards decision support systems enabling customised radiotherapy. Ra-diother. Oncol. 2013;109:159–164. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
