

Estimation of tumor size in breast cancer comparing clinical examination, mammography, ultrasound and MRI-correlation with the pathological analysis of the surgical specimen
- PMID: 28861372
- PMCID: PMC5566672
- DOI: 10.21037/gs.2017.03.09
Estimation of tumor size in breast cancer comparing clinical examination, mammography, ultrasound and MRI-correlation with the pathological analysis of the surgical specimen
Abstract
Background: To evaluate the best method in our center to measure preoperative tumor size in breast tumors, using as reference the tumor size in the postoperative surgical specimen. We compared physical examination vs. mammography vs. resonance vs. ultrasound. There are different studies in the literature with disparate results.
Methods: This is a retrospective study. All the included patients have been studied by clinical examination performed by gynecologist or surgeon specialists in senology, and radiological tests (mammography, ultrasound and magnetic resonance imaging). The correlation of mammary examination, ultrasound, mammography and resonance with pathological anatomy was studied using the Pearson index. Subsequently, the results of such imaging tests were compared with the tumor size of the infiltrating component measured by anatomopathological study using a student's t test for related variables. The level of significance was set at 95%. Statistical package R. was used.
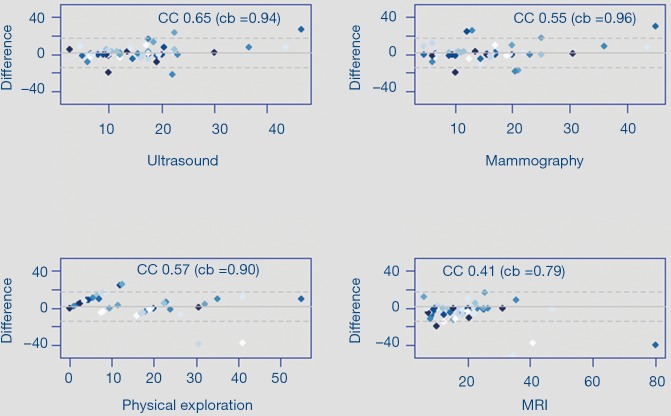
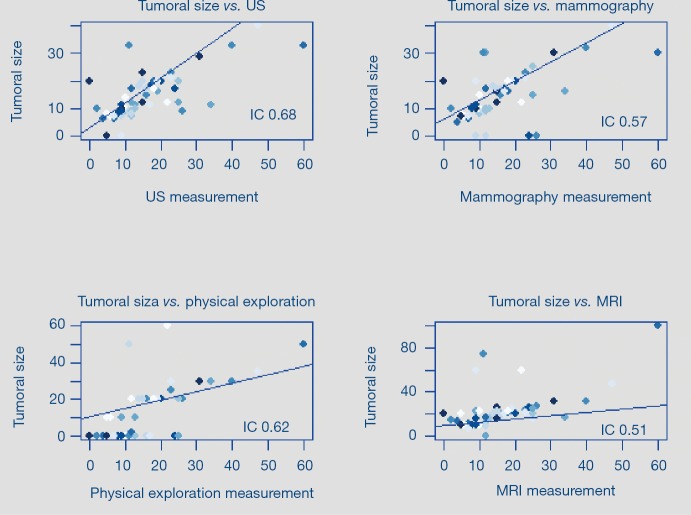
Results: A total of 73 cases were collected from October 2015 to July 2016 with diagnosis of infiltrating breast carcinoma. Twelve cases of carcinoma in situ and seven cases of neoadjuvant carcinoma are excluded. Finally, a total of 56 cases were included in the analysis. The mean age of the patients is 57 years. The histology is of infiltrating ductal carcinoma in 46 patients (80.7%), lobular in 8 (14%) and other carcinomas in 3 cases (5.2%). We verified the relationship between preoperative tumor size by physical examination, mammography, ultrasound (US) and magnetic resonance imaging (MRI), and the final size of the surgical specimen by applying a Pearson correlation test. A strong correlation was found between the physical examination results 0.62 (0.43-0.76 at 95% CI), ultrasound 0.68 (0.51-0.8 at 95% CI), mammography 0.57 (0.36-0.72 at 95% CI) and RM 0.51 (0.29-0.68 at 95% CI) with respect to pathological anatomy. The mean tumor size of the surgical specimen was 16.1 mm. Mean of tumor size by physical examination was 12.1 mm (P<0.05), by 14 mm US (P<0.05), by mammography of 14.3 (P<0.05) and by MRI of 22.53 mm (P>0.05).
Conclusions: Ultrasonography is the best predictor of tumor size in breast cancer, compared with clinical examination, mammography, and resonance. Our work could help the decision-making process such as the type of conservative surgery, the possible need for oncoplastic surgery or the decision to start treatment with neoadjuvant therapy, in patients with unifocal tumors.
Keywords: Breast cancer; magnetic resonance imaging (MRI); mammography; tumor size; ultrasound (US).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Feig SA. Breast masses. Mammographic and sonographic evaluation. Radiol Clin North Am 1992;30:67-92. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources