

Cystic adventitial disease-case series and review of literature
- PMID: 28861424
- PMCID: PMC5566729
- DOI: 10.21037/atm.2017.05.04
Cystic adventitial disease-case series and review of literature
Abstract
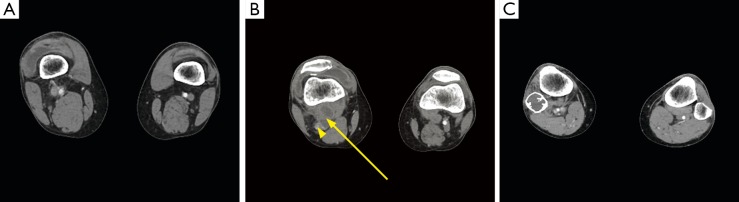
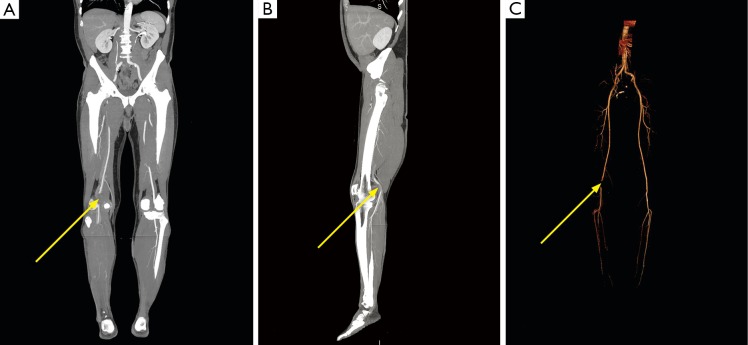
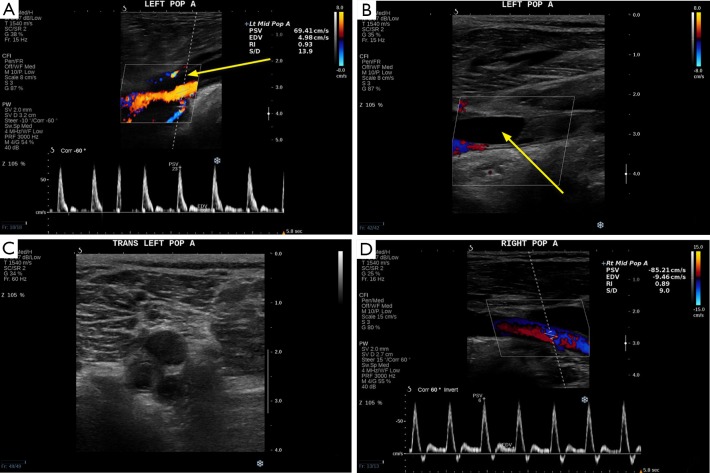
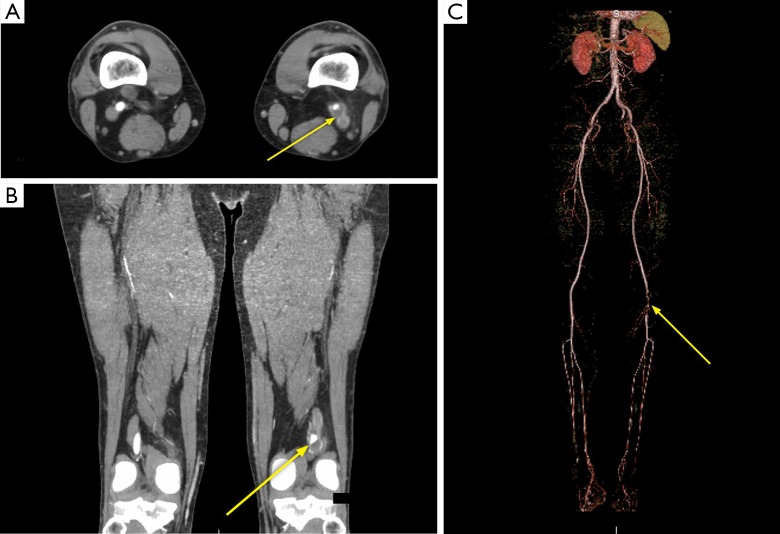
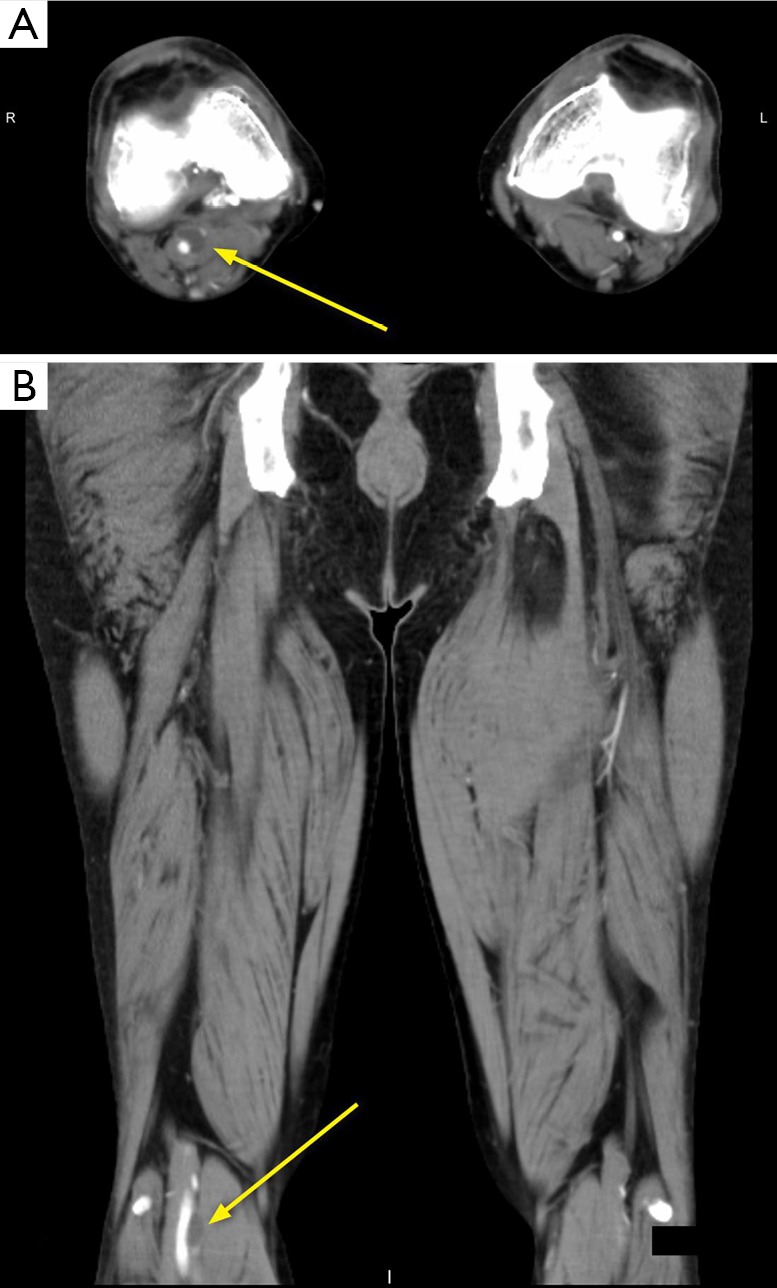
Cystic adventitial disease (CAD) is a rare vascular disorder that involves the arteries and rarely the veins, most commonly found in the popliteal artery of male patients. Etiology of CAD is uncertain and currently without a consensus agreement. Clinically, the most common presenting symptom is claudication. Diagnosis requires a strong clinical suspicion in patients with intermittent claudication, but without other risk factors for atherosclerotic disease. Angiography, ultrasound (US), computed tomography (CT) and magnetic resonance imaging (MRI) can all be used for diagnosis. Treatment of CAD can be done via surgical resection or percutaneous intervention such as aspiration. CAD can rarely recur after treatment.
Keywords: Cystic adventitial disease (CAD); Ishikawa sign; computed tomography angiography (CTA); scimitar sign; ultrasound (US).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous