

The complex relationship of exposure to new Plasmodium infections and incidence of clinical malaria in Papua New Guinea
- PMID: 28862132
- PMCID: PMC5606846
- DOI: 10.7554/eLife.23708
The complex relationship of exposure to new Plasmodium infections and incidence of clinical malaria in Papua New Guinea
Abstract
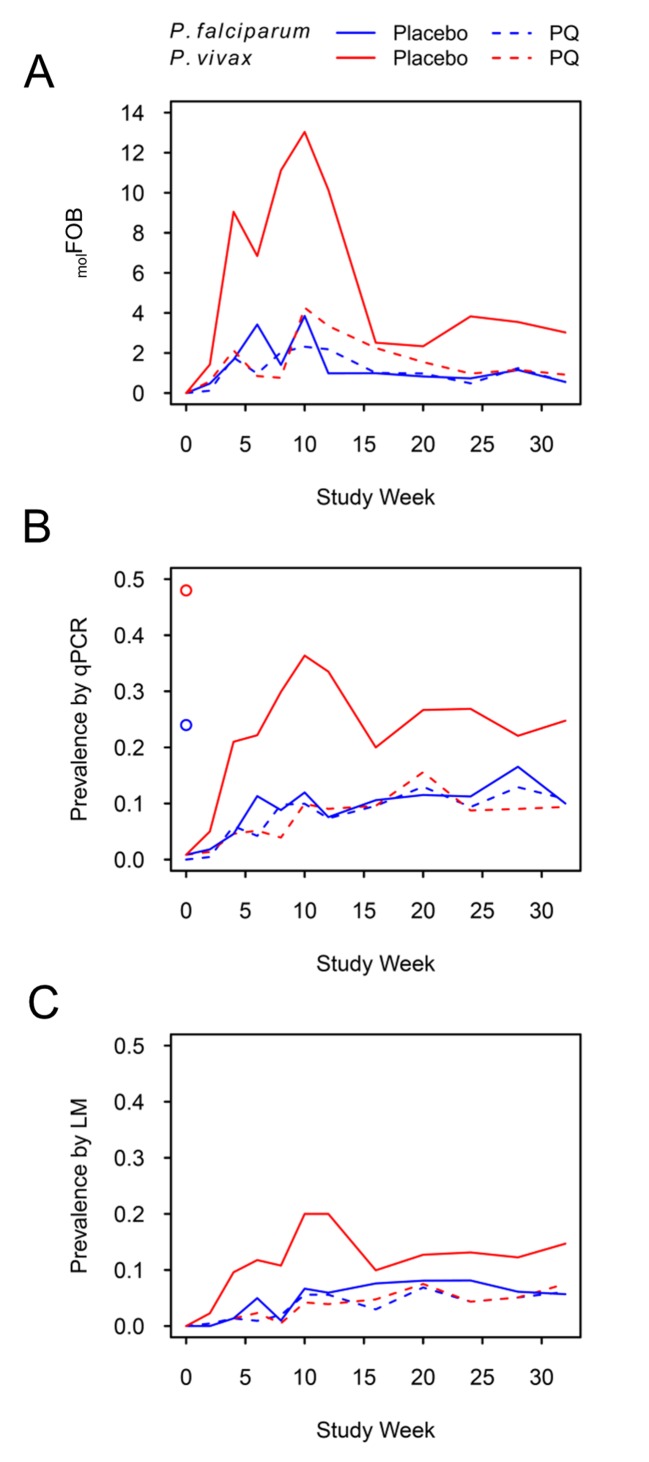
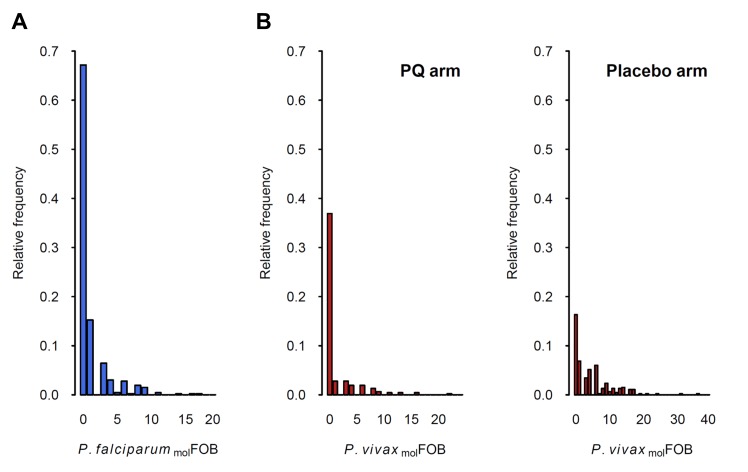
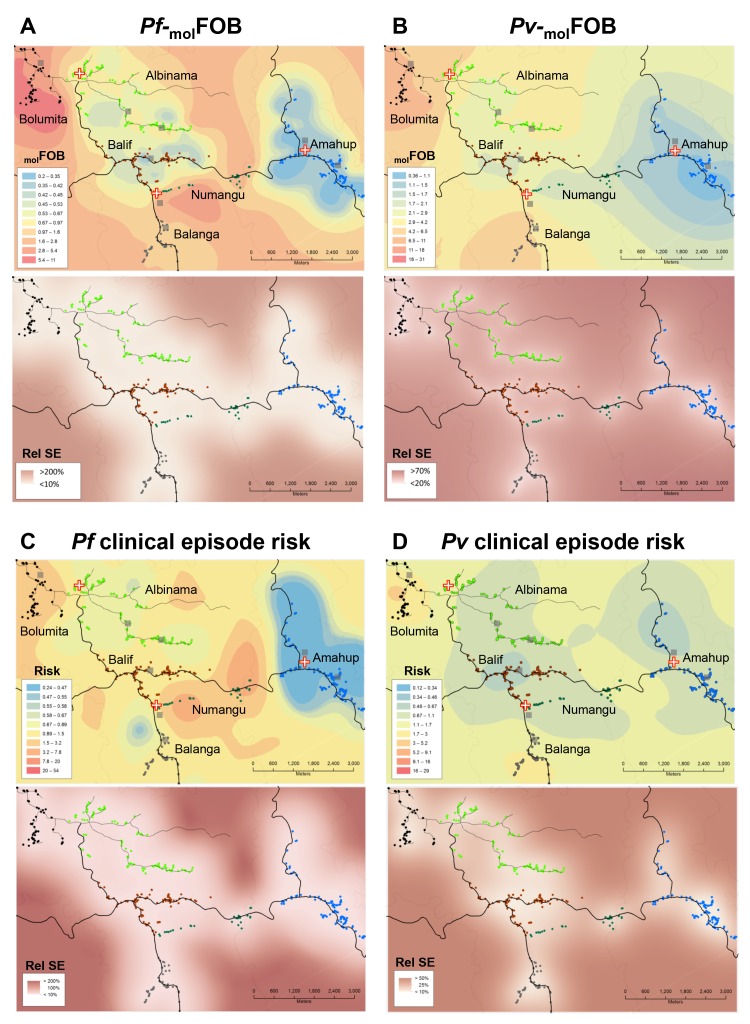
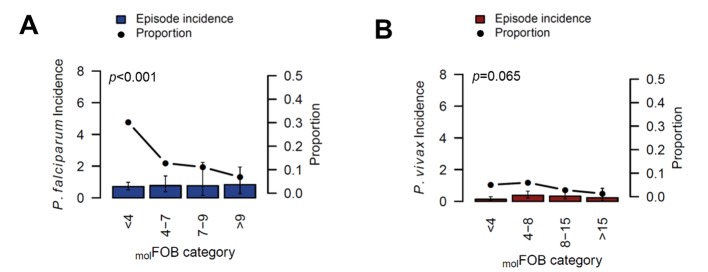
The molecular force of blood-stage infection (molFOB) is a quantitative surrogate metric for malaria transmission at population level and for exposure at individual level. Relationships between molFOB, parasite prevalence and clinical incidence were assessed in a treatment-to-reinfection cohort, where P.vivax (Pv) hypnozoites were eliminated in half the children by primaquine (PQ). Discounting relapses, children acquired equal numbers of new P. falciparum (Pf) and Pv blood-stage infections/year (Pf-molFOB = 0-18, Pv-molFOB = 0-23) resulting in comparable spatial and temporal patterns in incidence and prevalence of infections. Including relapses, Pv-molFOB increased >3 fold (relative to PQ-treated children) showing greater heterogeneity at individual (Pv-molFOB = 0-36) and village levels. Pf- and Pv-molFOB were strongly associated with clinical episode risk. Yearly Pf clinical incidence rate (IR = 0.28) was higher than for Pv (IR = 0.12) despite lower Pf-molFOB. These relationships between molFOB, clinical incidence and parasite prevalence reveal a comparable decline in Pf and Pv transmission that is normally hidden by the high burden of Pv relapses.
Clinical trial registration: ClinicalTrials.gov NCT02143934.
Keywords: p. falciparum; Papua New Guinea; Plasmodium vivax; epidemiology; global health; human; immunity; immunology; malaria; transmission.
Conflict of interest statement
No competing interests declared.
Figures
References
-
- Battle KE, Cameron E, Guerra CA, Golding N, Duda KA, Howes RE, Elyazar IR, Price RN, Baird JK, Reiner RC, Smith DL, Gething PW, Hay SI. Defining the relationship between plasmodium vivax parasite rate and clinical disease. Malaria Journal. 2015;14:191. doi: 10.1186/s12936-015-0706-3. - DOI - PMC - PubMed
-
- Betuela I, Rosanas-Urgell A, Kiniboro B, Stanisic DI, Samol L, de Lazzari E, Del Portillo HA, Siba P, Alonso PL, Bassat Q, Mueller I. Relapses contribute significantly to the risk of plasmodium vivax infection and disease in papua new guinean children 1-5 years of age. The Journal of Infectious Diseases. 2012;206:1771–1780. doi: 10.1093/infdis/jis580. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
