

Lateral canthotomy orbitotomy: a rapid approach to the orbit
- PMID: 28862259
- PMCID: PMC5811693
- DOI: 10.1038/eye.2017.173
Lateral canthotomy orbitotomy: a rapid approach to the orbit
Abstract
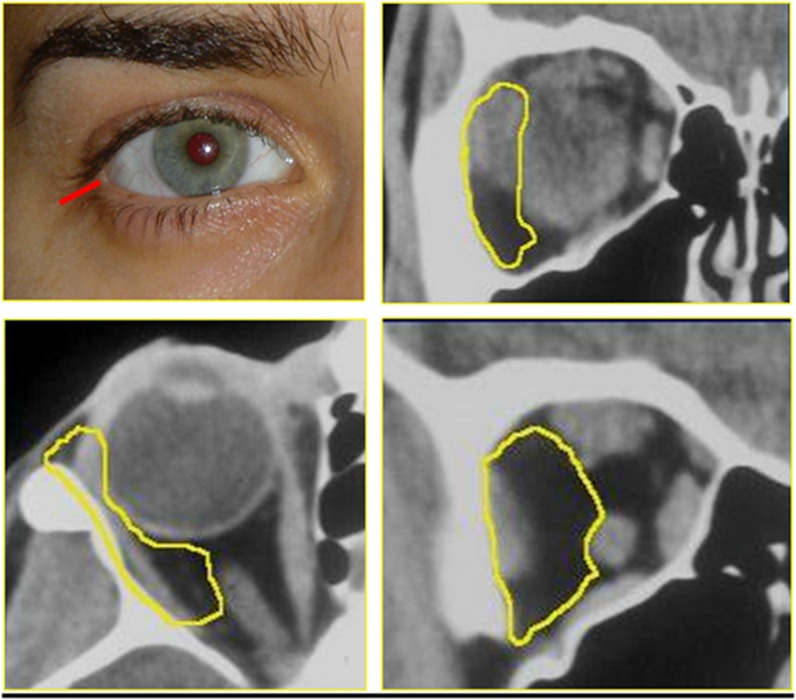
PurposeThe lateral compartment of the orbit can readily be accessed through a horizontal lateral canthotomy without the need to swing the lid or remove bone. In this paper the technique, accessible orbital territory, and duration of surgery are presented.Patients and methodsRetrospective, non-interventional descriptive case series for patients who underwent a lateral canthotomy to access pathology within the lateral orbit.ResultsA series of 18 patients are included, all presenting with pathology lateral to, or within, the optic nerve. Pathologies included amyloidosis (1), lymphoma (4), metastatic adenocarcinoma within the optic nerve (1), idiopathic lateral rectus muscle mysositis (4), meningothelial meningioma of the optic nerve (1), intraconal orbital meningioma (1), reactive lymphoid hyperplasia (1), optic nerve glioma (3), optic nerve meningioma (1), and cavernous haemangioma (1). The median surgical time was 36 min (range 23-75 min). No patient required detachment of the lower lid, the technique leaving both upper and lower 'arms' of the lateral canthal tendon attached to Whitnall's tubercle.ConclusionsThe lateral canthotomy approach orbitotomy is a rapid, safe, and minimally disruptive approach for accessing pathology in the lateral orbit and optic nerve. The lateral canthal tendon is split along the horizontal raphe without detachment of either limb from Whitnall's tubercle, no bone is removed, and the post-operative recovery is rapid with minimal associated inflammation or chemosis. This approach is also flexible, permitting the clinician to increase exposure to the orbit peroperatively by swinging the lower lid if required.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Kronlein RU. Zur pathologie und operative behandlung der dermoidcysten der orbita. Bruns Beitr Klin Chir 1888; 4: 149–163.
-
- Berke RN. Modified Kronlein operation. AMA Arch Ophthalmol 1954; 51: 609–632. - PubMed
-
- Reese AB. Orbital tumors and their surgical treatment. Am J Ophthalmol 1941; 24: 386–394497-502.
-
- Smith JL. Anterolateral approach to the orbit. Trans Am Acad Ophthalmol Otolaryngol 1971; 75: 1059–1064. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
