

Better glycaemic control and less hypoglycaemia with insulin glargine 300 U/mL vs glargine 100 U/mL: 1-year patient-level meta-analysis of the EDITION clinical studies in people with type 2 diabetes
- PMID: 28862801
- PMCID: PMC5836995
- DOI: 10.1111/dom.13105
Better glycaemic control and less hypoglycaemia with insulin glargine 300 U/mL vs glargine 100 U/mL: 1-year patient-level meta-analysis of the EDITION clinical studies in people with type 2 diabetes
Abstract
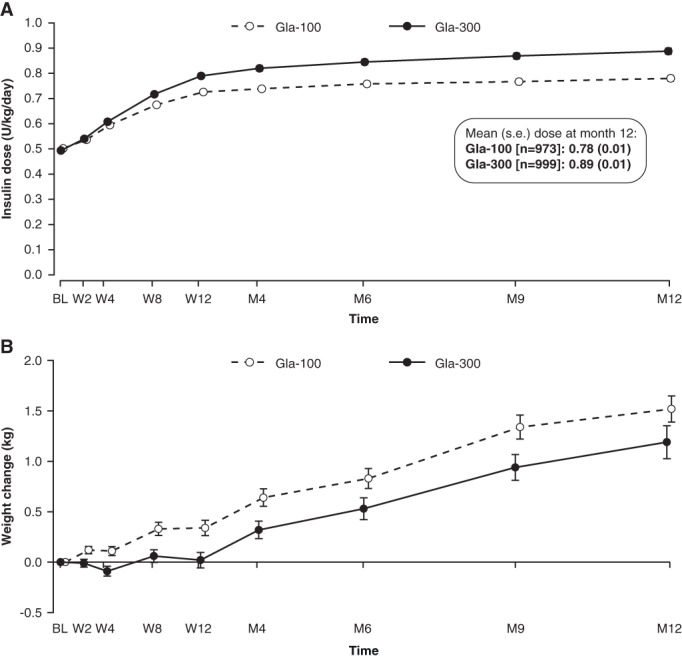
Aims: To investigate the efficacy and safety of insulin glargine 300 U/mL (Gla-300) vs insulin glargine 100 U/mL (Gla-100) over 12 months in a patient-level meta-analysis, using data from the EDITION studies in people with type 2 diabetes (T2DM).
Methods: EDITION 1, 2 and 3 were multicentre, randomized, open-label, 2-arm, parallel-group, treat-to-target phase IIIa studies. Similar study designs and endpoints enabled a meta-analysis to be conducted.
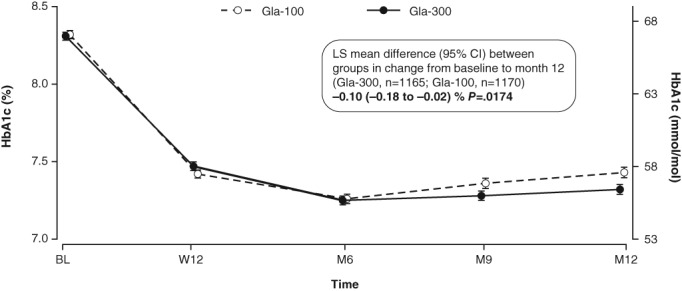
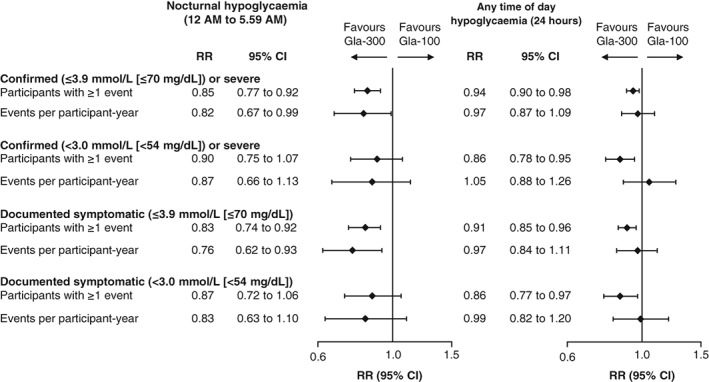
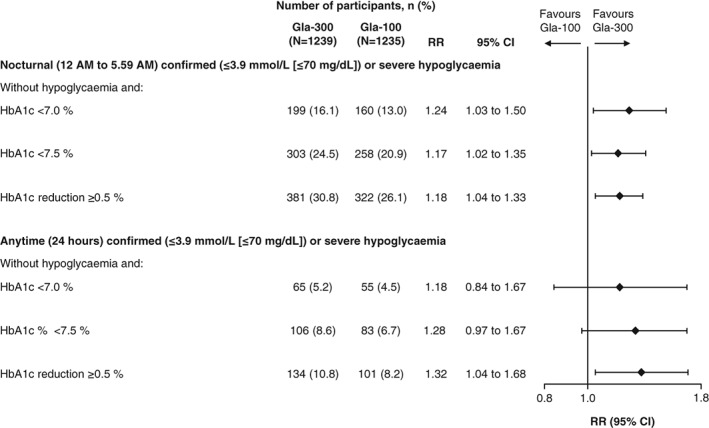
Results: Reductions in glycated haemoglobin (HbA1c) were better sustained over 12 months with Gla-300 than with Gla-100 (least squares [LS] mean difference in change from baseline: -0.10 % [95% confidence interval {CI} -0.18 to -0.02] or -1.09 mmol/mol [95% CI -2.01 to -0.20]; P = .0174). Risk of confirmed (≤3.9 mmol/L) or severe hypoglycaemia was 15% lower with Gla-300 vs Gla-100 at night (relative risk 0.85 [95% CI 0.77-0.92]) and 6% lower at any time of day (relative risk 0.94 [95% CI 0.90-0.98]). Rates of hypoglycaemia were 18% lower with Gla-300 vs Gla-100 at night (rate ratio 0.82 [95% CI 0.67-0.99]), but comparable at any time of day. HbA1c <7.0 % without nocturnal hypoglycaemia was achieved by 24% more participants with Gla-300 than with Gla-100 (relative risk 1.24 [95% CI 1.03-1.50]). Severe hypoglycaemia was rare; in both treatment groups the incidence of events at any time of day was ≤3.6%, while rates were ≤0.08 events per participant-year.
Conclusions: In a broad population of people with T2DM over 12 months, use of Gla-300 provided more sustained glycaemic control and significantly lower hypoglycaemia risk at night and at any time of day compared with Gla-100.
Keywords: glycaemic control; hypoglycaemia; insulin analogues; meta-analysis; phase III study; type 2 diabetes.
© 2017 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
R. Ritzel has served as a consultant for AstraZeneca, Merck (MSD), Novo Nordisk, Servier and Sanofi and on the speakers bureau for AstraZeneca, Bristol‐Myers Squibb, Eli Lilly, Merck (MSD), Novartis, Novo Nordisk and Sanofi. R. Roussel has served on advisory panels for AstraZeneca, Eli Lilly and Physiogenex, as a board member for Janssen, Merck (MSD), Novo Nordisk, Sanofi, and as a consultant for Eli Lilly, and has received research support from Amgen and Sanofi. A. G. has served as a consultant for AstraZeneca, Boehringer Ingelheim, Eli Lilly, Sanofi and Takeda, has received research support from AstraZeneca and Merck (MSD), and has served on the speakers bureau for AstraZeneca. J. V. has received research support and served on the advisory panel and speakers bureau for Abbott, AstraZeneca, Boehringer Ingelheim, Bristol‐Myers Squibb, Eli Lilly, GlaxoSmithKline, Merck (MSD), Novartis, Novo Nordisk, Roche, Sanofi and Takeda. C. B.‐W. is an employee of Sanofi. H. Y.‐J. has served on the advisory panel for Eli Lilly, Merck (MSD) and Sanofi, and as a consultant for Eli Lilly and Sanofi.
Figures
Similar articles
-
Patient-level meta-analysis of the EDITION 1, 2 and 3 studies: glycaemic control and hypoglycaemia with new insulin glargine 300 U/ml versus glargine 100 U/ml in people with type 2 diabetes.Diabetes Obes Metab. 2015 Sep;17(9):859-67. doi: 10.1111/dom.12485. Epub 2015 Jun 16. Diabetes Obes Metab. 2015. PMID: 25929311 Free PMC article.
-
New insulin glargine 300 U/ml versus glargine 100 U/ml in Japanese people with type 2 diabetes using basal insulin and oral antihyperglycaemic drugs: glucose control and hypoglycaemia in a randomized controlled trial (EDITION JP 2).Diabetes Obes Metab. 2016 Apr;18(4):366-74. doi: 10.1111/dom.12618. Epub 2016 Jan 21. Diabetes Obes Metab. 2016. PMID: 26662838 Free PMC article. Clinical Trial.
-
One-year sustained glycaemic control and less hypoglycaemia with new insulin glargine 300 U/ml compared with 100 U/ml in people with type 2 diabetes using basal plus meal-time insulin: the EDITION 1 12-month randomized trial, including 6-month extension.Diabetes Obes Metab. 2015 Sep;17(9):835-42. doi: 10.1111/dom.12472. Epub 2015 May 11. Diabetes Obes Metab. 2015. PMID: 25846721 Free PMC article. Clinical Trial.
-
Effectiveness of insulin glargine U-300 versus insulin glargine U-100 on nocturnal hypoglycemia and glycemic control in type 1 and type 2 diabetes: a systematic review and meta-analysis.Acta Diabetol. 2019 Mar;56(3):355-364. doi: 10.1007/s00592-018-1258-0. Epub 2018 Dec 3. Acta Diabetol. 2019. PMID: 30506484
-
A review of the safety and efficacy data for insulin glargine 300 units/ml, a new formulation of insulin glargine.Diabetes Obes Metab. 2015 Dec;17(12):1107-14. doi: 10.1111/dom.12531. Epub 2015 Sep 10. Diabetes Obes Metab. 2015. PMID: 26139151 Review.
Cited by
-
Second-Generation Insulin Analogues - a Review of Recent Real-World Data and Forthcoming Head-to-Head Comparisons.Eur Endocrinol. 2018 May;14(Suppl1):2-9. doi: 10.17925/EE.2018.14supp1.2. Epub 2018 May 11. Eur Endocrinol. 2018. PMID: 30034546 Free PMC article. Review.
-
Glargine-300: An updated literature review on randomized controlled trials and real-world studies.World J Diabetes. 2020 Apr 15;11(4):100-114. doi: 10.4239/wjd.v11.i4.100. World J Diabetes. 2020. PMID: 32313609 Free PMC article. Review.
-
The Current Situation Regarding Long-Acting Insulin Analogues Including Biosimilars Among African, Asian, European, and South American Countries; Findings and Implications for the Future.Front Public Health. 2021 Jun 24;9:671961. doi: 10.3389/fpubh.2021.671961. eCollection 2021. Front Public Health. 2021. PMID: 34249838 Free PMC article.
-
Redefining Hypoglycemia in Clinical Trials: Validation of Definitions Recently Adopted by the American Diabetes Association/European Association for the Study of Diabetes.Diabetes Care. 2020 Feb;43(2):398-404. doi: 10.2337/dc18-2361. Epub 2019 Oct 28. Diabetes Care. 2020. PMID: 31658975 Free PMC article.
-
Insulin Glargine 300 U/mL and Insulin Glulisine Treatment in Patients with Type 2 Diabetes: A Non-Interventional Study of Effectiveness in Routine Clinical Practice.Diabetes Ther. 2020 Feb;11(2):467-478. doi: 10.1007/s13300-019-00746-4. Epub 2020 Jan 3. Diabetes Ther. 2020. PMID: 31901115 Free PMC article.
References
-
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient‐centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140–149. - PubMed
-
- Donnelly LA, Morris AD, Evans JM. Adherence to insulin and its association with glycaemic control in patients with type 2 diabetes. QJM. 2007;100(6):345–350. - PubMed
-
- Becker RH, Dahmen R, Bergmann K, Lehmann A, Jax T, Heise T. New insulin glargine 300 Units·mL−1 provides a more even activity profile and prolonged glycemic control at steady state compared with insulin glargine 100 Units·mL−1. Diabetes Care. 2015;38(4):637–643. - PubMed
-
- Bergenstal RM, Bailey TS, Rodbard D, et al. Comparison of insulin glargine 300 U/mL and 100 U/mL in adults with type 1 diabetes: continuous glucose monitoring profiles and variability using morning or evening injections. Diabetes Care. 2017;40(4):554–560. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
