

A Systems Biology Approach to Investigating Sex Differences in Cardiac Hypertrophy
- PMID: 28862954
- PMCID: PMC5586433
- DOI: 10.1161/JAHA.117.005838
A Systems Biology Approach to Investigating Sex Differences in Cardiac Hypertrophy
Abstract
Background: Heart failure preceded by hypertrophy is a leading cause of death, and sex differences in hypertrophy are well known, although the basis for these sex differences is poorly understood.
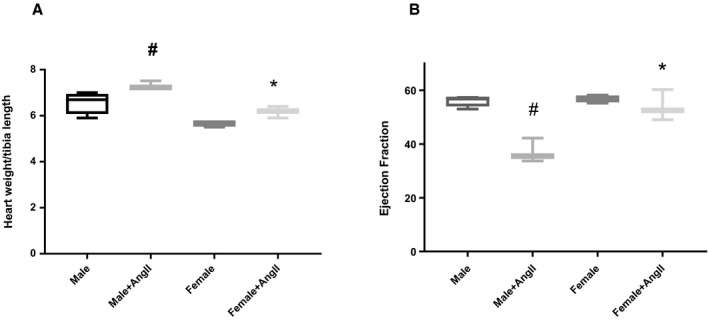
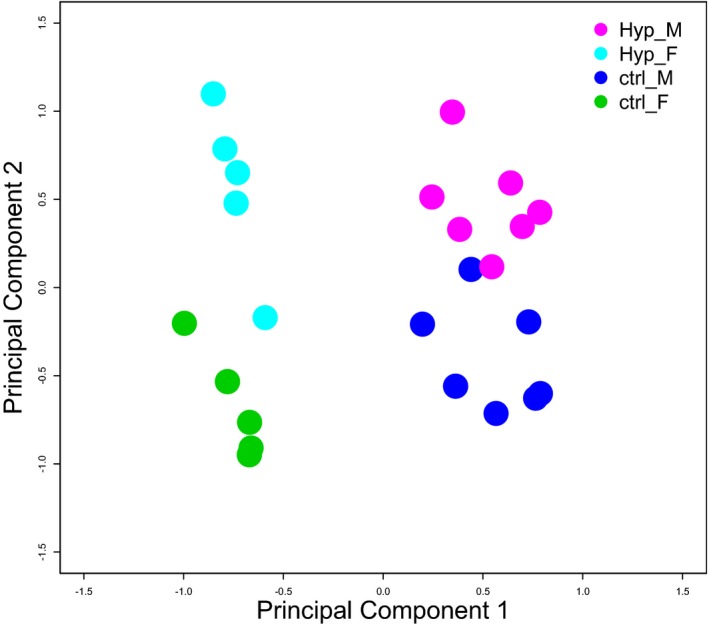
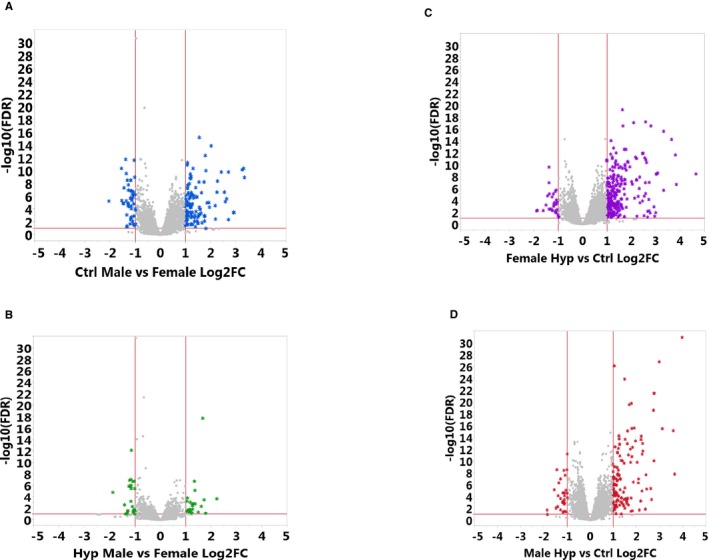
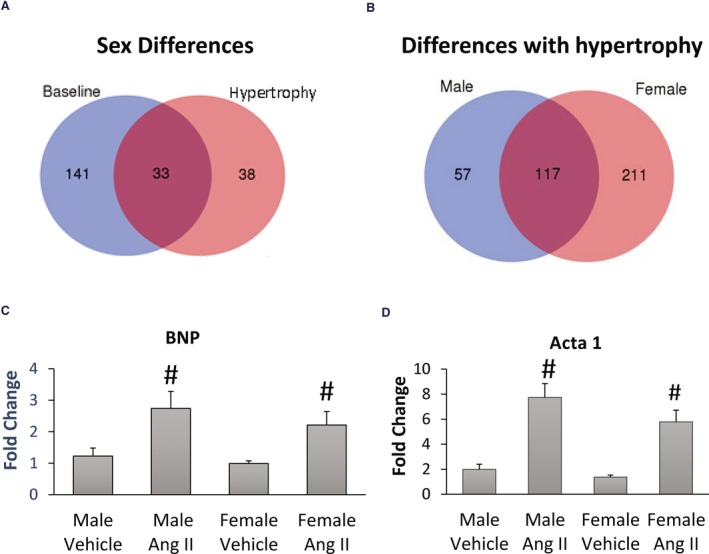
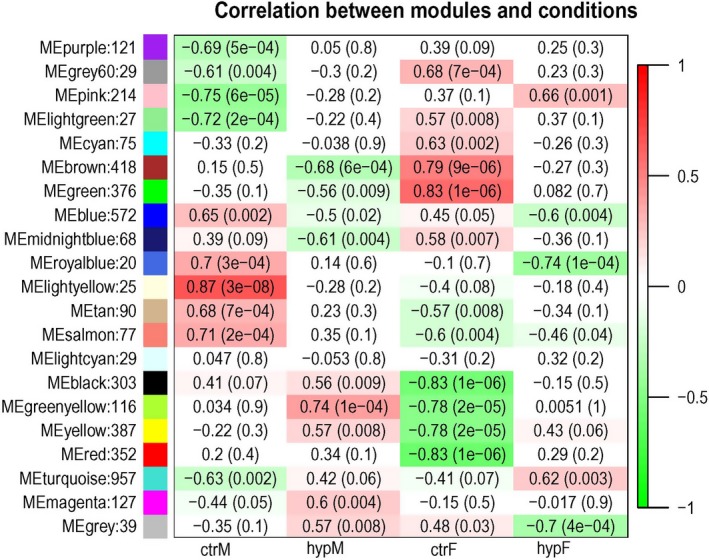
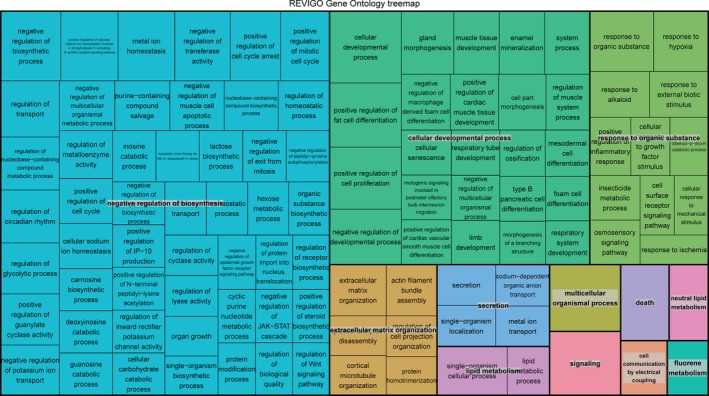
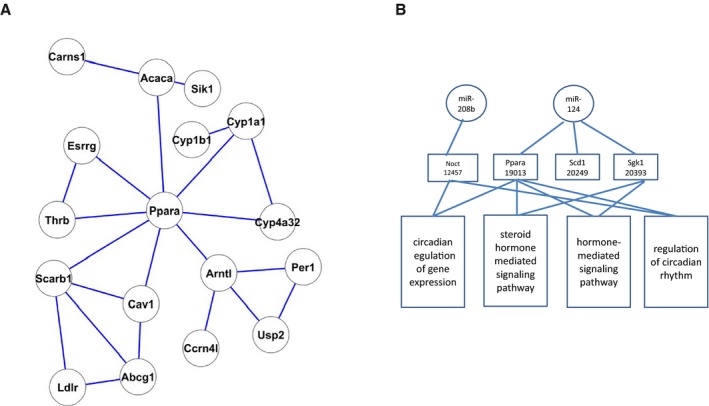
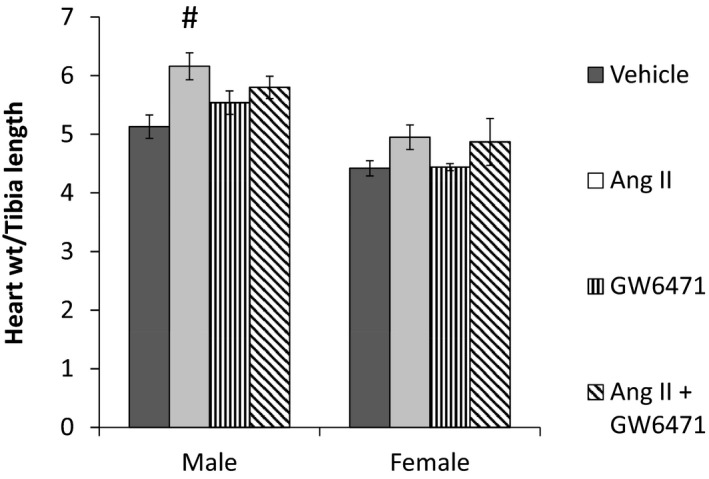
Methods and results: This study used a systems biology approach to investigate mechanisms underlying sex differences in cardiac hypertrophy. Male and female mice were treated for 2 and 3 weeks with angiotensin II to induce hypertrophy. Sex differences in cardiac hypertrophy were apparent after 3 weeks of treatment. RNA sequencing was performed on hearts, and sex differences in mRNA expression at baseline and following hypertrophy were observed, as well as within-sex differences between baseline and hypertrophy. Sex differences in mRNA were substantial at baseline and reduced somewhat with hypertrophy, as the mRNA differences induced by hypertrophy tended to overwhelm the sex differences. We performed an integrative analysis to identify mRNA networks that were differentially regulated in the 2 sexes by hypertrophy and obtained a network centered on PPARα (peroxisome proliferator-activated receptor α). Mouse experiments further showed that acute inhibition of PPARα blocked sex differences in the development of hypertrophy.
Conclusions: The data in this study suggest that PPARα is involved in the sex-dimorphic regulation of cardiac hypertrophy.
Keywords: hypertrophy; sex; systems biology.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Barrett‐Connor E. Sex differences in coronary heart disease. Why are women so superior? The 1995 Ancel Keys Lecture. Circulation. 1997;95:252–264. - PubMed
-
- Hayward CS, Kelly RP, Collins P. The roles of gender, the menopause and hormone replacement on cardiovascular function. Cardiovasc Res. 2000;46:28–49. - PubMed
-
- Krumholz HM, Larson M, Levy D. Sex differences in cardiac adaptation to isolated systolic hypertension. Am J Cardiol. 1993;72:310–313. - PubMed
-
- Lee DS, Gona P, Vasan RS, Larson MG, Benjamin EJ, Wang TJ, Tu JV, Levy D. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation. 2009;119:3070–3077. - PMC - PubMed
-
- Scantlebury DC, Borlaug BA. Why are women more likely than men to develop heart failure with preserved ejection fraction? Curr Opin Cardiol. 2011;26:562–568. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
