

Invasive lobular carcinoma of the breast: A special histological type compared with invasive ductal carcinoma
- PMID: 28863134
- PMCID: PMC5580913
- DOI: 10.1371/journal.pone.0182397
Invasive lobular carcinoma of the breast: A special histological type compared with invasive ductal carcinoma
Abstract
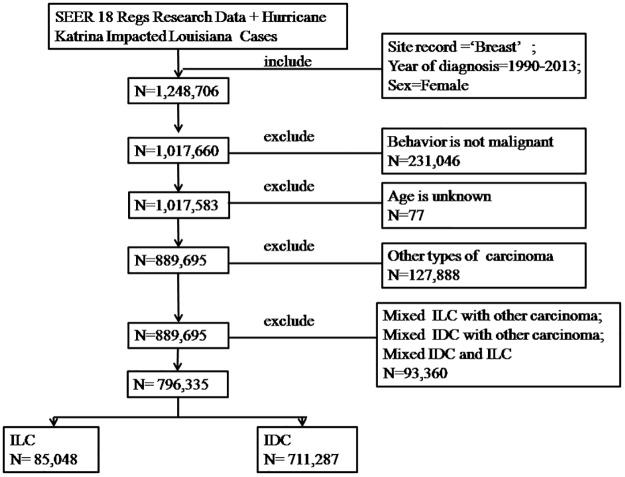
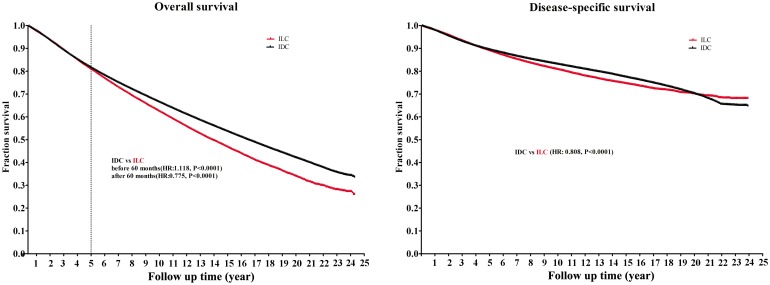
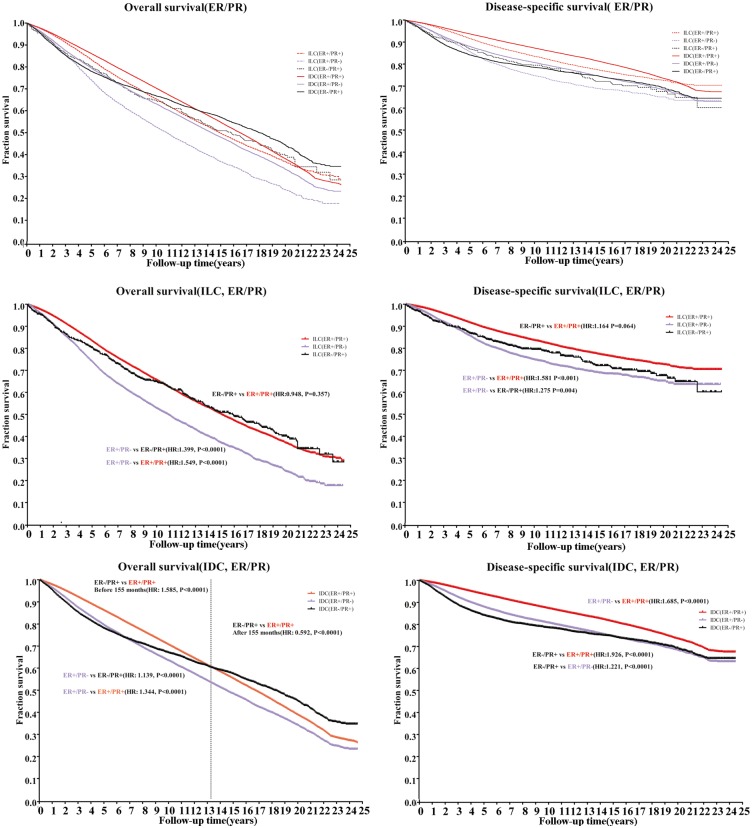
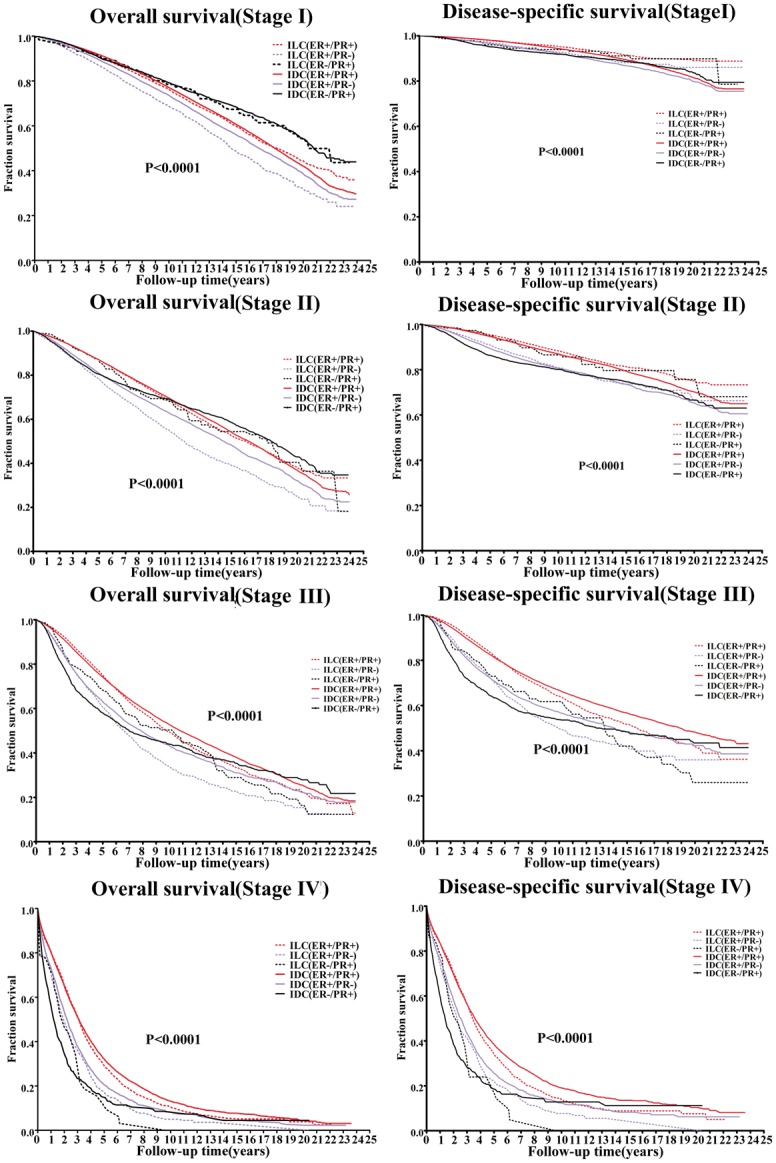
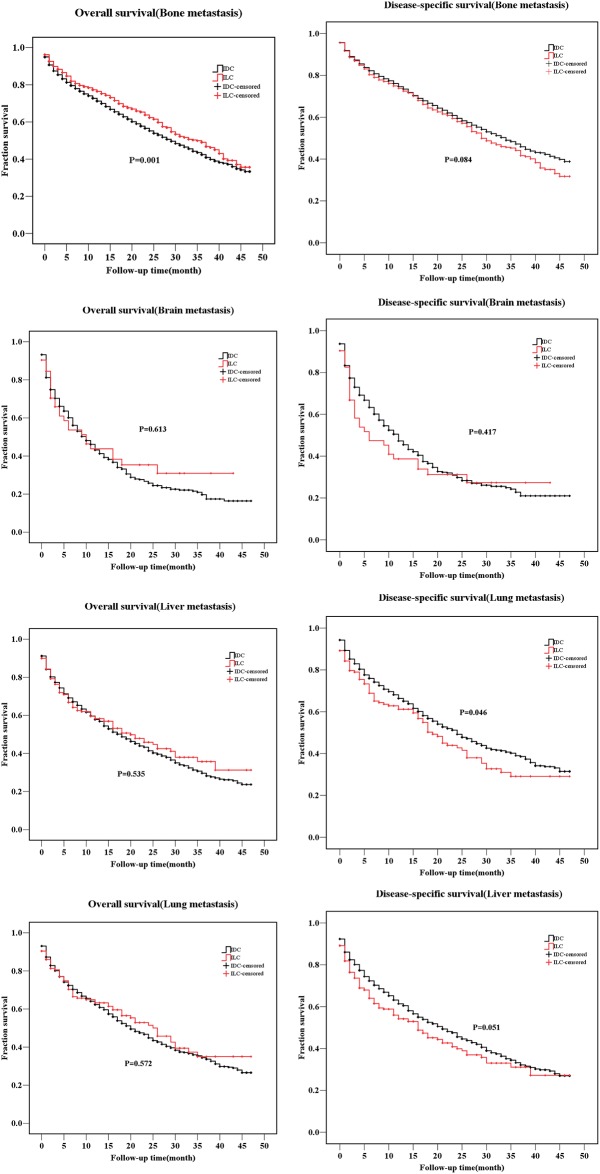
The clinical outcomes and therapeutic strategies for infiltrating ductal carcinoma (IDC) and infiltrating lobular carcinoma (ILC) are not uniform. The primary objectives of this study were to identify the differences in the clinical characteristics and prognoses between ILC and IDC, and identify the high-risk population based on the hormone receptor status and metastasis sites. The Surveillance, Epidemiology, and End Results Program database was searched and patients diagnosed with ILC or IDC from 1990 to 2013 were identified. In total,796,335 patients were analyzed, including 85,048 withILC (10.7%) and 711,287 withIDC (89.3%). The ILC group was correlatedwith older age, larger tumor size, later stage, lower grade, metastasis disease(M1) disease, and greater counts ofpositive lymph nodesandestrogen-receptor-positive (ER)/progesterone receptor-positive (PR) positive nodes. The overall survival showed an early advantage for ILC but a worse outcome after 5 years. Regarding the disease-specific survival, the IDC cohort had advantages over the ILC group, both during the early years and long-term. In hormone status and metastasis site subgroup analyses, the ER+/PR+ subgroup had the best survival, while the ER+/PR- subgroup had the worst outcome, especially the ILC cohort. ILC and IDC had different metastasis patterns. The proportion of bone metastasis was higher in the ILC group (91.52%) than that in the IDC (76.04%), and the ILC group was more likely to have multiple metastasis sites. Survival analyses showed patients with ILC had a higher risk of liver metastasis (disease-specific survival[DSS]; P = 0.046), but had a better overall survival than the bone metastasis group (P<0.0001). We concluded that the long-term prognosis for ILC was poorer than that for IDC, and the ER+/PR- subgroup had the worst outcome. Therefore, the metastasis pattern and prognosis must be seriously evaluated, and a combination of endocrine therapy and chemotherapy should be considered.
Conflict of interest statement
Figures
References
-
- Anderson WF, Matsuno R. Breast cancer heterogeneity: a mixture of at least two main types? Journal of the National Cancer Institute. 2006;98(14):948–51. doi: 10.1093/jnci/djj295 . - DOI - PubMed
-
- McCart Reed AE, Kutasovic JR, Lakhani SR, Simpson PT. Invasive lobular carcinoma of the breast: morphology, biomarkers and 'omics. Breast cancer research: BCR. 2015;17:12 doi: 10.1186/s13058-015-0519-x . - DOI - PMC - PubMed
-
- Guiu S, Wolfer A, Jacot W, Fumoleau P, Romieu G, Bonnetain F, et al. Invasive lobular breast cancer and its variants: how special are they for systemic therapy decisions? Critical reviews in oncology/hematology. 2014;92(3):235–57. doi: 10.1016/j.critrevonc.2014.07.003 . - DOI - PubMed
-
- Wong SM, Freedman RA, Sagara Y, Stamell EF, Desantis SD, Barry WT, et al. The effect of Paget disease on axillary lymph node metastases and survival in invasive ductal carcinoma. Cancer. 2015;121(24):4333–40. doi: 10.1002/cncr.29687 . - DOI - PubMed
-
- Nelson RA, Guye ML, Luu T, Lai LL. Survival outcomes of metaplastic breast cancer patients: results from a US population-based analysis. Annals of surgical oncology. 2015;22(1):24–31. doi: 10.1245/s10434-014-3890-4 . - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
