

Glioblastoma targeted therapy: updated approaches from recent biological insights
- PMID: 28863449
- PMCID: PMC5834086
- DOI: 10.1093/annonc/mdx106
Glioblastoma targeted therapy: updated approaches from recent biological insights
Abstract
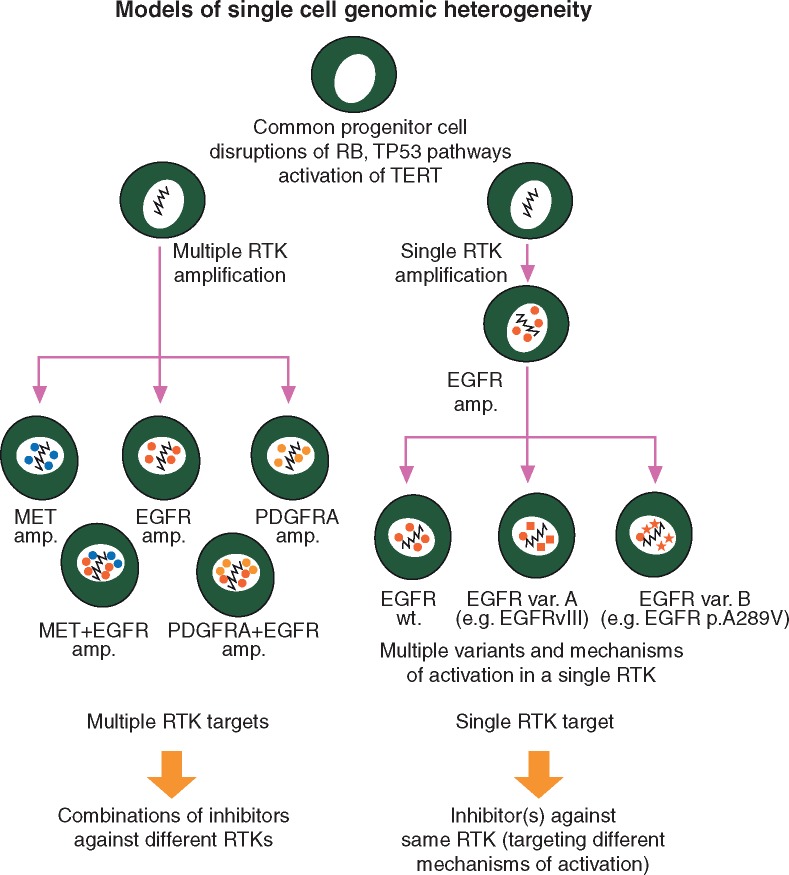
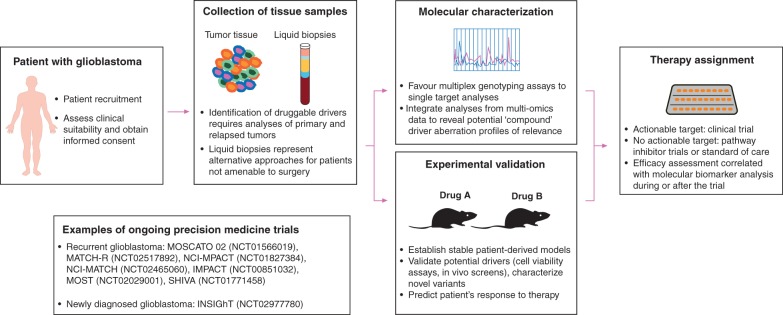
Glioblastoma (WHO grade IV astrocytoma) is the most frequent primary brain tumor in adults, representing a highly heterogeneous group of neoplasms that are among the most aggressive and challenging cancers to treat. An improved understanding of the molecular pathways that drive malignancy in glioblastoma has led to the development of various biomarkers and the evaluation of several agents specifically targeting tumor cells and the tumor microenvironment. A number of rational approaches are being investigated, including therapies targeting tumor growth factor receptors and downstream pathways, cell cycle and epigenetic regulation, angiogenesis and antitumor immune response. Moreover, recent identification and validation of prognostic and predictive biomarkers have allowed implementation of modern trial designs based on matching molecular features of tumors to targeted therapeutics. However, while occasional targeted therapy responses have been documented in patients, to date no targeted therapy has been formally validated as effective in clinical trials. The lack of knowledge about relevant molecular drivers in vivo combined with a lack of highly bioactive and brain penetrant-targeted therapies remain significant challenges. In this article, we review the most promising biological insights that have opened the way for the development of targeted therapies in glioblastoma, and examine recent data from clinical trials evaluating targeted therapies and immunotherapies. We discuss challenges and opportunities for the development of these agents in glioblastoma.
Keywords: biomarkers; cancer genomics; glioma; personalized medicine; precision medicine; targeted therapies.
© The Author 2017. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ. et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005; 352: 987–996. - PubMed
-
- Stupp R, Taillibert S, Kanner AA. et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: a randomized clinical trial. JAMA 2015; 314: 2535–2543. - PubMed
-
- Weller M, van den Bent M, Hopkins K. et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol 2014; 15: e395–e403. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
