

Quality Gaps and Comparative Effectiveness of Management Strategies for Recurrent Malignant Pleural Effusions
- PMID: 28864054
- PMCID: PMC6743066
- DOI: 10.1016/j.chest.2017.08.026
Quality Gaps and Comparative Effectiveness of Management Strategies for Recurrent Malignant Pleural Effusions
Abstract
Background: Guidelines for recurrent malignant pleural effusions (MPEs) recommend definitive procedures, such as indwelling pleural catheters (IPCs) or pleurodesis, over repeat thoracentesis. We hypothesized that many patients have multiple thoracenteses rather than definitive procedures and that this results in more procedures and complications.
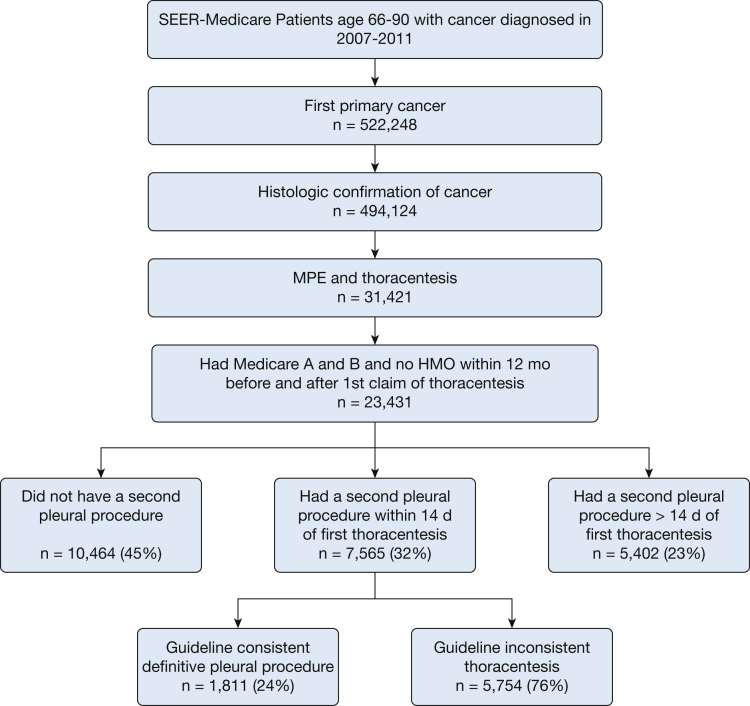
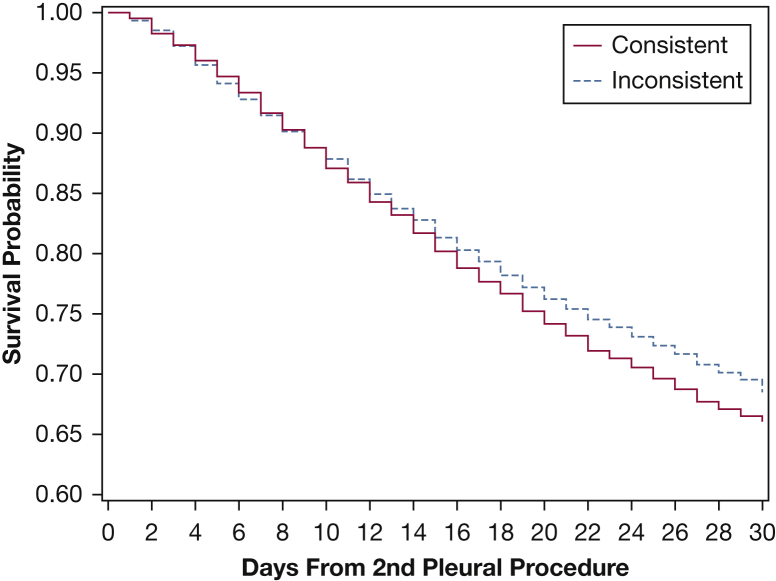
Methods: Retrospective cohort study using SEER-Medicare data from 2007 to 2011. Patients 66 to 90 years of age with an MPE were included. The primary outcome was whether patients with rapidly recurring MPE, defined as recurrence within 2 weeks of first thoracentesis, received guideline consistent care. Guideline consistent care was defined as a definitive second pleural procedure.
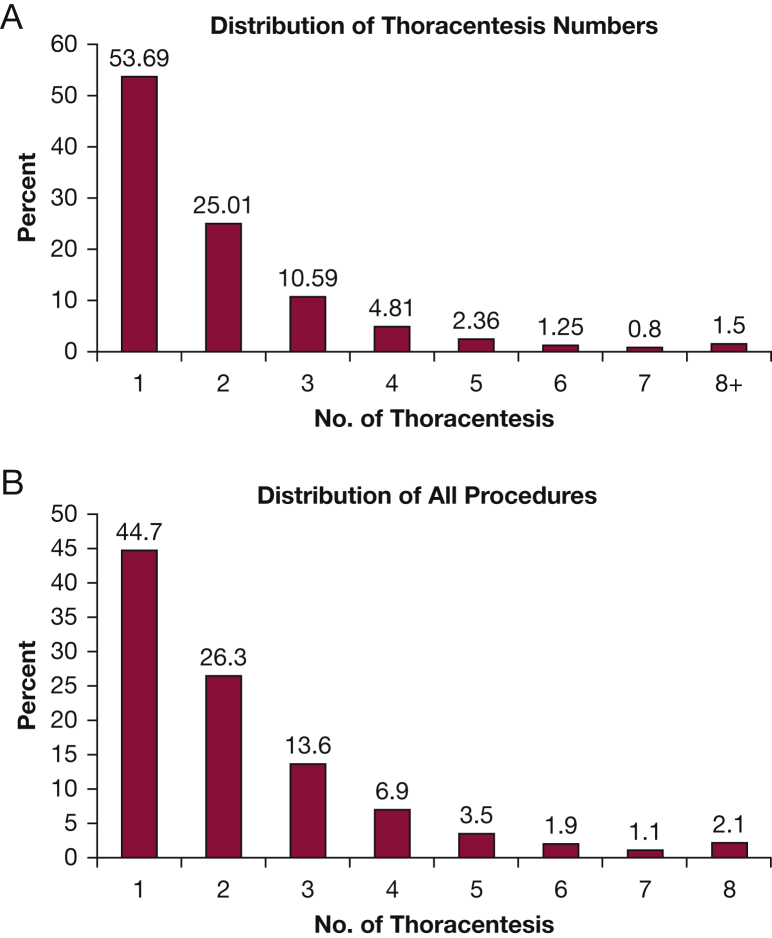
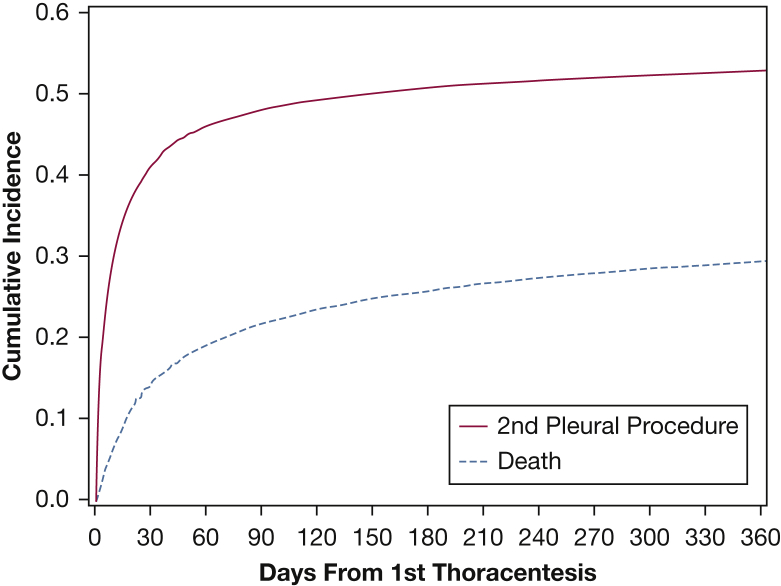
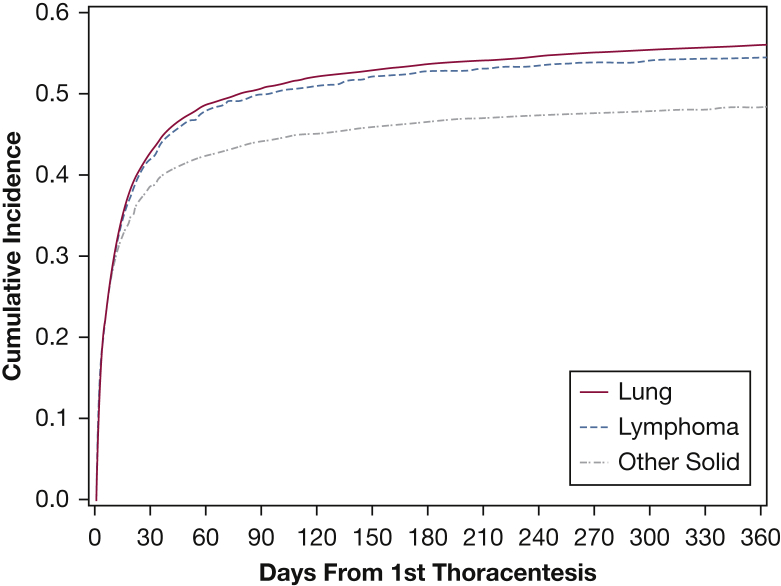
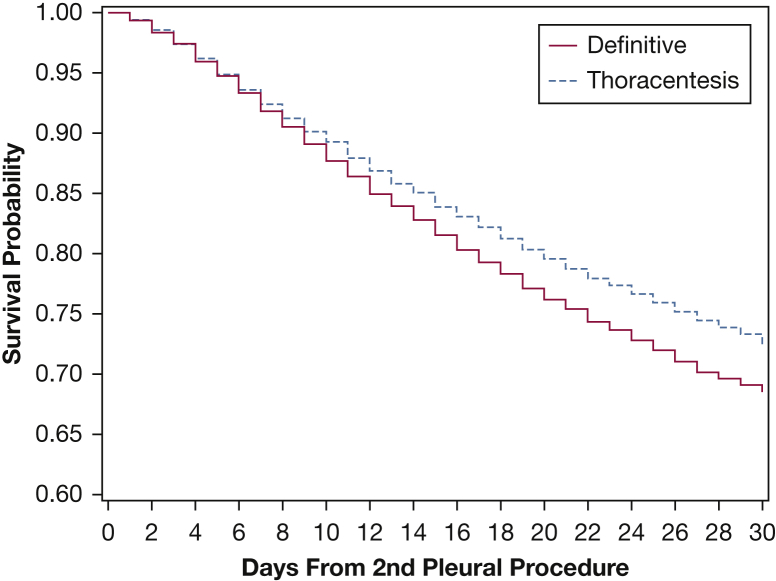
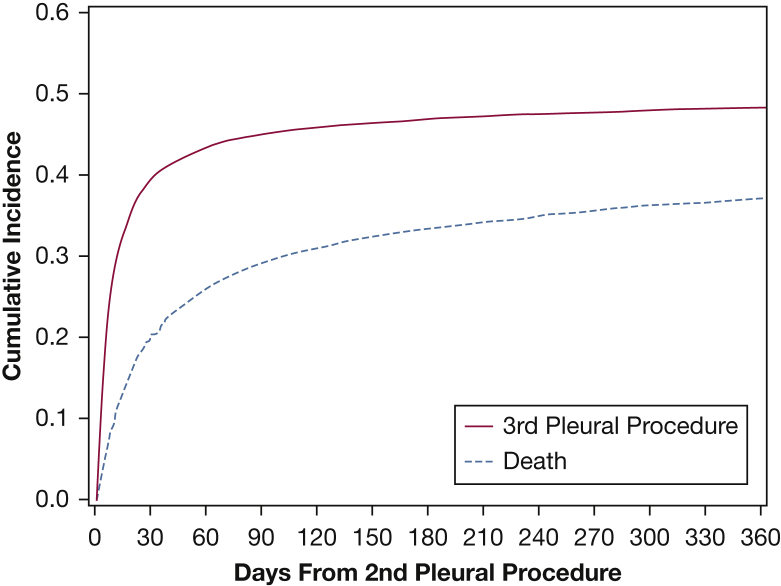
Results: Thoracentesis for MPE was performed in 23,431 patients. A second pleural procedure because of recurrence was required in 12,967 (55%). Recurrence was rapid in 7,565 (58%) of the 12,967 patients that had a recurrence. Of the 7,565 patients with rapid recurrence, 1,811 (24%) received guideline consistent care. Definitive pleural procedures compared with repeat thoracentesis resulted in fewer subsequent pleural procedures (0.62 vs 1.44 procedures per patient, respectively; P < .0001), fewer pneumothoraxes (< 0.0037 vs 0.009 pneumothoraxes per patient, respectively; P = .001), and fewer ED procedures (0.02 vs 0.04 ED procedures per patient, respectively; P < .001). Repeat thoracentesis and IPCs resulted in fewer inpatient days compared with chest tube or thoracoscopic pleurodesis (0.013 vs 0.013 vs 0.085 vs 0.097 inpatient days per day of life, respectively; P < .001).
Conclusions: Guideline consistent care using definitive procedures compared with repeat thoracentesis was associated with fewer subsequent procedures and complications; however, pleurodesis resulted in more inpatient days.
Keywords: indwelling pleural catheter; malignant pleural effusion; pleural effusion; pleurodesis; thoracentesis; thoracoscopy.
Copyright © 2017. Published by Elsevier Inc.
Figures
Comment in
-
Interventional Pulmonology-Bridging the Gaps through Standardization: Malignant Pleural Effusion, Mediastinal Staging, and Cryobiopsy.Am J Respir Crit Care Med. 2018 Jun 1;197(11):1478-1480. doi: 10.1164/rccm.201711-2274RR. Am J Respir Crit Care Med. 2018. PMID: 29583020 No abstract available.
Similar articles
-
The Clinical and Economic Implications of Different Treatment Pathways for Patients With Rapidly Recurrent Malignant Pleural Effusion.Chest. 2024 Oct;166(4):867-881. doi: 10.1016/j.chest.2024.04.036. Epub 2024 Jun 3. Chest. 2024. PMID: 38838953
-
Procedures Performed during Hospitalizations for Malignant Pleural Effusions: Data from the 2012 National Inpatient Sample.Respiration. 2018;95(4):228-234. doi: 10.1159/000485934. Epub 2018 Feb 7. Respiration. 2018. PMID: 29414821
-
Indwelling pleural catheters reduce inpatient days over pleurodesis for malignant pleural effusion.Chest. 2012 Aug;142(2):394-400. doi: 10.1378/chest.11-2657. Chest. 2012. PMID: 22406960
-
Recent developments in pleurodesis for malignant pleural disease.Clin Respir J. 2018 Oct;12(10):2463-2468. doi: 10.1111/crj.12958. Clin Respir J. 2018. PMID: 30252207 Review.
-
Update on the diagnosis and management of malignant pleural effusions.Respir Med. 2022 May;196:106802. doi: 10.1016/j.rmed.2022.106802. Epub 2022 Mar 9. Respir Med. 2022. PMID: 35287006 Review.
Cited by
-
Contemporary best practice in the management of malignant pleural effusion.Ther Adv Respir Dis. 2018 Jan-Dec;12:1753466618785098. doi: 10.1177/1753466618785098. Ther Adv Respir Dis. 2018. PMID: 29952251 Free PMC article. Review.
-
Lymph nodes rather than pleural metabolic activity in 18F-FDG PET/CT correlates with malignant pleural effusion recurrence in advanced non-small cell lung cancer.Transl Lung Cancer Res. 2024 Sep 30;13(9):2236-2253. doi: 10.21037/tlcr-24-291. Epub 2024 Sep 25. Transl Lung Cancer Res. 2024. PMID: 39430341 Free PMC article.
-
ATS Core Curriculum 2021. Adult Pulmonary Medicine: Thoracic Oncology.ATS Sch. 2021 Sep 1;2(3):468-483. doi: 10.34197/ats-scholar.2021-0032RE. eCollection 2021 Sep. ATS Sch. 2021. PMID: 34667994 Free PMC article.
-
Pleural effusions in hematologic malignancies and their management with indwelling pleural catheters.Curr Opin Pulm Med. 2018 Jul;24(4):384-391. doi: 10.1097/MCP.0000000000000490. Curr Opin Pulm Med. 2018. PMID: 29629920 Free PMC article. Review.
-
Cost Comparison of Treatment Alternatives for Pleural Effusion and Ascites from a Payer Perspective: Are There Cost Savings from Indwelling Catheters?J Palliat Med. 2023 Nov;26(11):1510-1520. doi: 10.1089/jpm.2022.0592. Epub 2023 Jun 23. J Palliat Med. 2023. PMID: 37352428 Free PMC article.
References
-
- Antony V.B., Loddenkemper R., Astoul P. Management of malignant pleural effusions. Eur Respir J. 2001;18(2):402–419. - PubMed
-
- Rodriguez-Panadero F., Borderas Naranjo F., Lopez Mejias J. Pleural metastatic tumours and effusions. Frequency and pathogenic mechanisms in a post-mortem series. Eur Respir J. 1989;2(4):366–369. - PubMed
-
- Roberts M.E., Neville E., Berrisford R.G., Antunes G., Ali N.J., Group BTSPDG Management of a malignant pleural effusion: British Thoracic Society Pleural Disease Guideline 2010. Thorax. 2010;65(suppl 2):ii32–ii40. - PubMed
-
- Simoff M.J., Lally B., Slade M.G. Symptom management in patients with lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 suppl):e455S–497S. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
