

An immune clock of human pregnancy
- PMID: 28864494
- PMCID: PMC5701281
- DOI: 10.1126/sciimmunol.aan2946
An immune clock of human pregnancy
Abstract
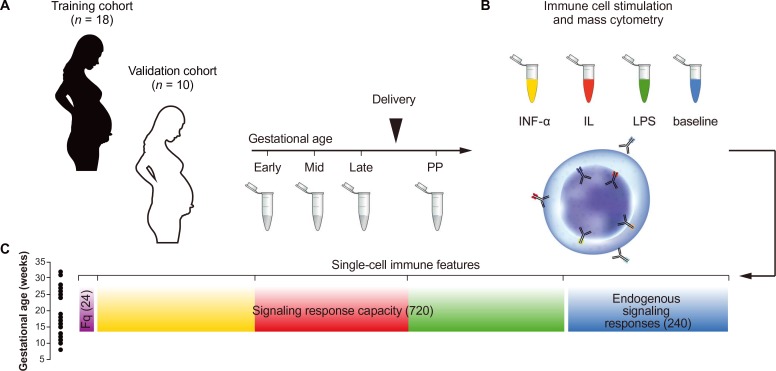
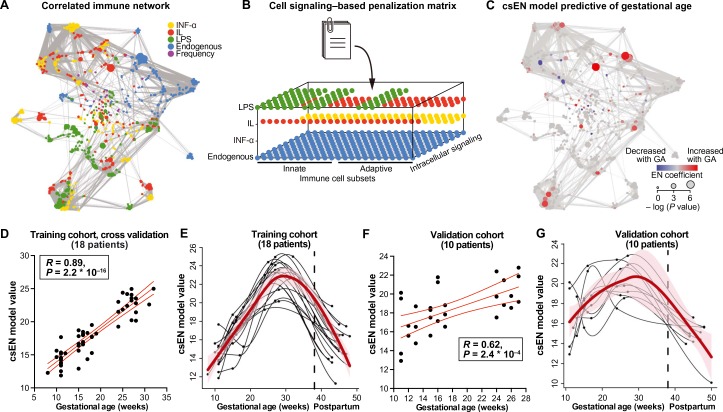
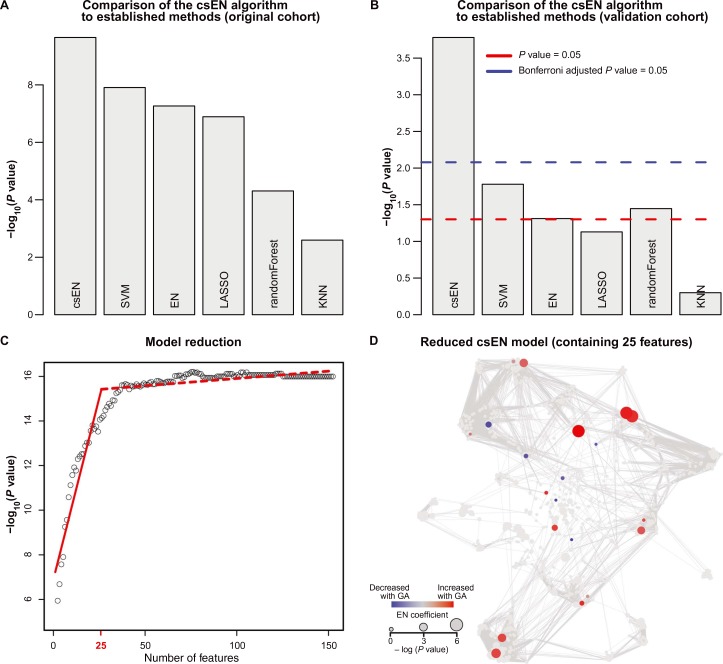
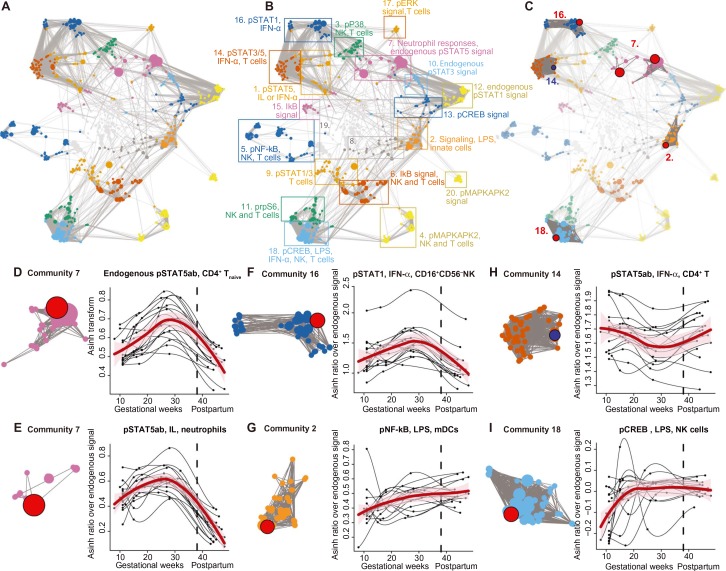
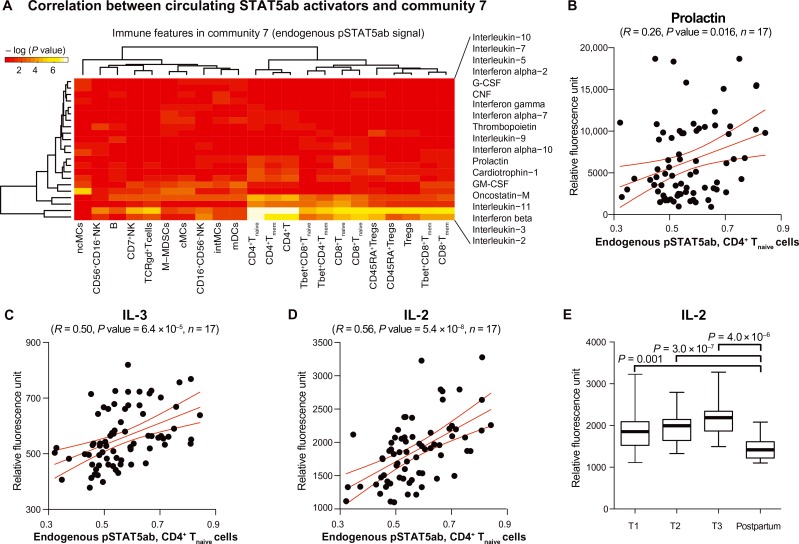
The maintenance of pregnancy relies on finely tuned immune adaptations. We demonstrate that these adaptations are precisely timed, reflecting an immune clock of pregnancy in women delivering at term. Using mass cytometry, the abundance and functional responses of all major immune cell subsets were quantified in serial blood samples collected throughout pregnancy. Cell signaling-based Elastic Net, a regularized regression method adapted from the elastic net algorithm, was developed to infer and prospectively validate a predictive model of interrelated immune events that accurately captures the chronology of pregnancy. Model components highlighted existing knowledge and revealed previously unreported biology, including a critical role for the interleukin-2-dependent STAT5ab signaling pathway in modulating T cell function during pregnancy. These findings unravel the precise timing of immunological events occurring during a term pregnancy and provide the analytical framework to identify immunological deviations implicated in pregnancy-related pathologies.
Copyright © 2017 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution License 4.0 (CC BY).
Conflict of interest statement
G.P.N. has equity in Fluidigm and Becton Dickinson, the manufacturers that produce the reagents or instrumentation used in this manuscript. The other authors declare that they have no competing interests.
Figures
Comment in
-
Pregnancy Around the Clock.Trends Mol Med. 2018 Jan;24(1):1-3. doi: 10.1016/j.molmed.2017.11.007. Epub 2017 Dec 5. Trends Mol Med. 2018. PMID: 29203370
References
-
- Erlebacher A., Immunology of the maternal-fetal interface. Annu. Rev. Immunol. 31, 387–411 (2013). - PubMed
-
- PrabhuDas M., Bonney E., Caron K., Dey S., Erlebacher A., Fazleabas A., Fisher S., Golos T., Matzuk M., McCune J. M., Mor G., Schulz L., Soares M., Spencer T., Strominger J., Way S. S., Yoshinaga K., Immune mechanisms at the maternal-fetal interface: Perspectives and challenges. Nat. Immunol. 16, 328–334 (2015). - PMC - PubMed
-
- Arck P. C., Hecher K., Fetomaternal immune cross-talk and its consequences for maternal and offspring’s health. Nat. Med. 99, 548–556 (2013). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
