

Extracellular histones are clinically relevant mediators in the pathogenesis of acute respiratory distress syndrome
- PMID: 28865478
- PMCID: PMC5581408
- DOI: 10.1186/s12931-017-0651-5
Extracellular histones are clinically relevant mediators in the pathogenesis of acute respiratory distress syndrome
Abstract
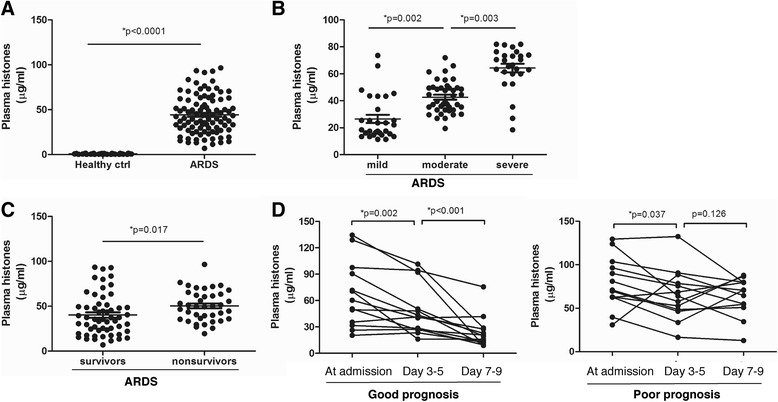
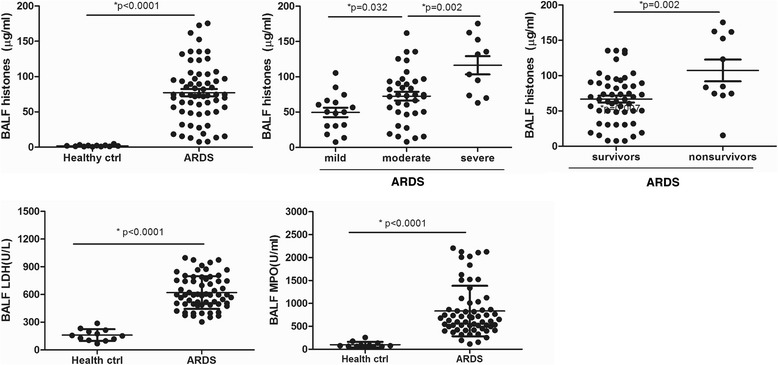
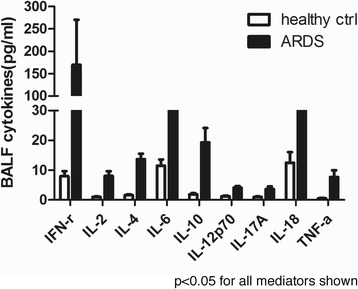
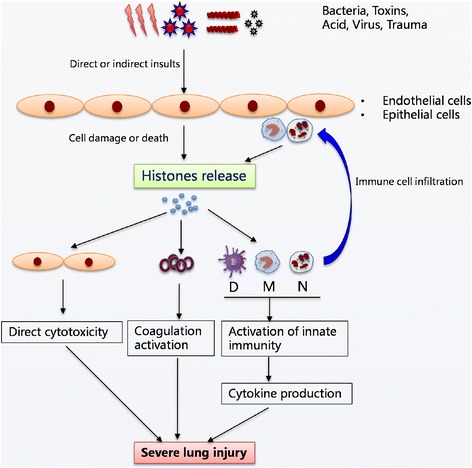
Background: Extracellular histones were recently identified as an inflammatory mediator involved in the pathogenesis of various organ injuries. This study aimed to examine extracellular histone levels and their clinical implications in acute respiratory distress syndrome (ARDS) patients and to explore histone-mediated effects through ex-vivo investigations.
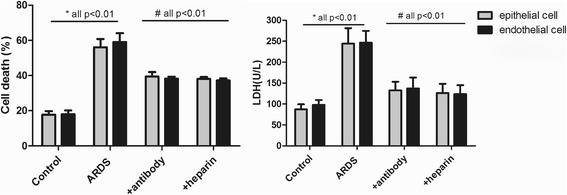
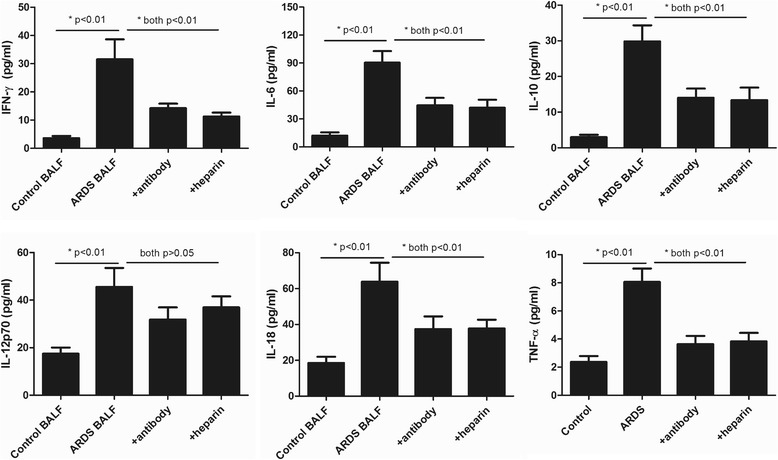
Methods: Extracellular histones, cytokine profiles and clinical data from 96 ARDS patients and 30 healthy volunteers were obtained. Human bronchial epithelial cells (BEAS-2B), human pulmonary artery endothelial cells (HPAEC), and human monocytic U937 cells were exposed to bronchoalveolar lavage fluid (BALF) collected from ARDS patients, and cellular damage and cytokine production were assessed. Furthermore, the effect of histone-targeted interventions by heparin or anti-histone antibody was evaluated.
Results: Plasma and BALF extracellular histone levels were much higher in ARDS patients than in healthy controls. There was a significant association between extracellular histones and ARDS severity and mortality. In addition, extracellular histones correlated with an evident systemic inflammation detected in ARDS patients. Ex-vivo analysis further showed that ARDS patient's BALF remarkably induced epithelial and endothelial cell damage and stimulated cytokine production in the supernatant of U937 cells. The adverse effects on these cells could be abrogated by heparin or anti-histone antibody.
Conclusions: Extracellular histones in ARDS patients are excessively increased and may contribute to disease aggravation by inducing cellular damage and promoting systemic inflammation. Targeting extracellular histones may provide a promising approach for treating ARDS.
Keywords: Acute respiratory distress syndrome (ARDS); Cell damage; Extracellular histones; Systemic inflammation.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Shanghai Pulmonary Hospital, Tongji University School of Medicine (Shanghai, P.R.China).
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
