

Recent advances in assays for the fragile X-related disorders
- PMID: 28866801
- PMCID: PMC5769695
- DOI: 10.1007/s00439-017-1840-5
Recent advances in assays for the fragile X-related disorders
Abstract
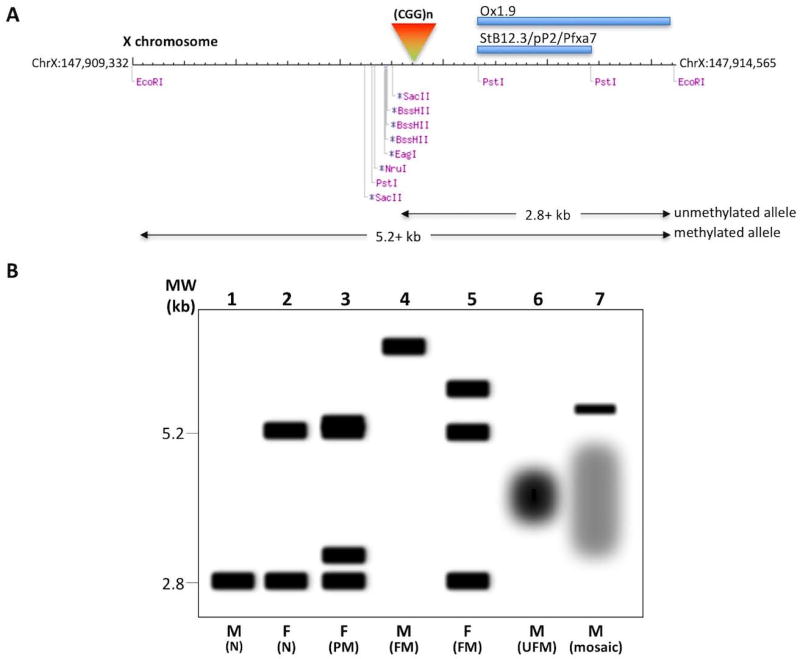
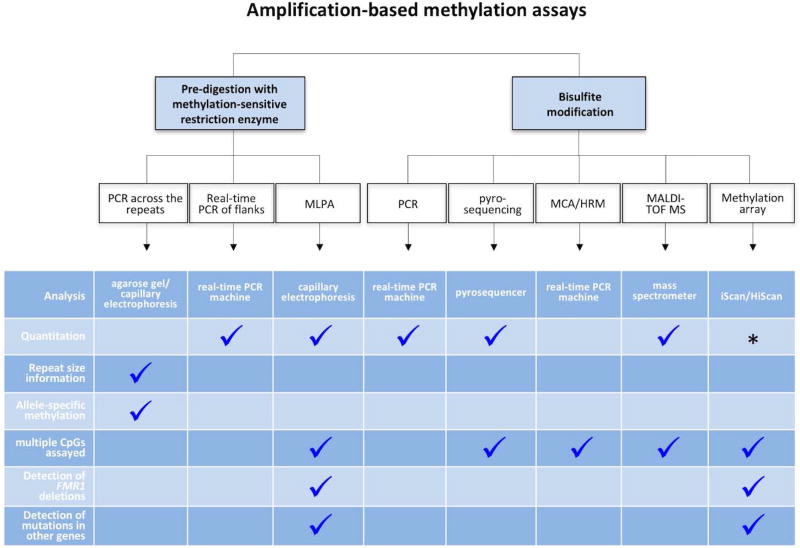
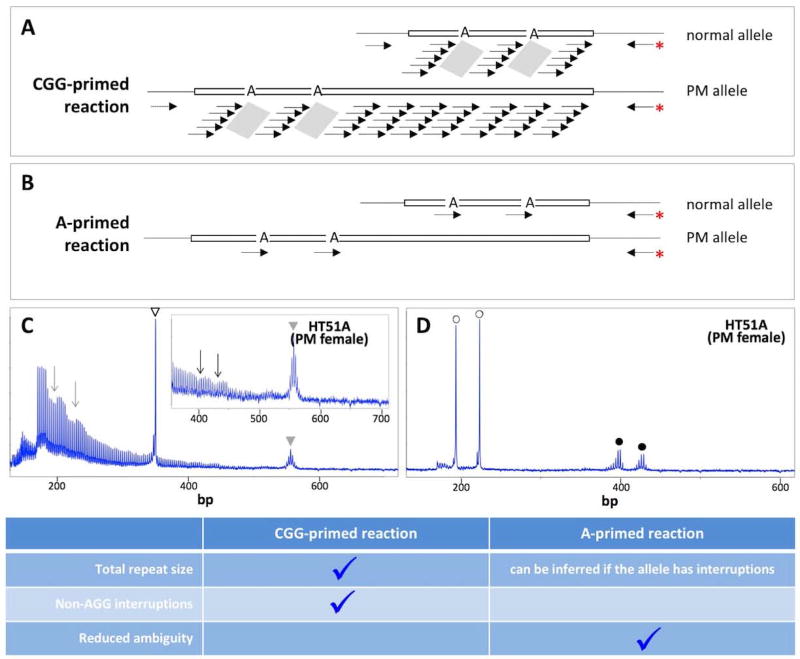
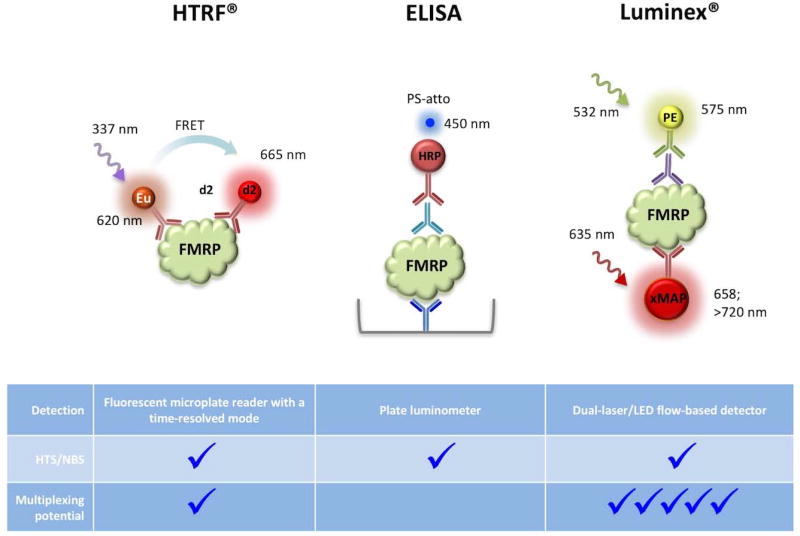
The fragile X-related disorders are a group of three clinical conditions resulting from the instability of a CGG-repeat tract at the 5' end of the FMR1 transcript. Fragile X-associated tremor/ataxia syndrome (FXTAS) and fragile X-associated primary ovarian insufficiency (FXPOI) are disorders seen in carriers of FMR1 alleles with 55-200 repeats. Female carriers of these premutation (PM) alleles are also at risk of having a child who has an FMR1 allele with >200 repeats. Most of these full mutation (FM) alleles are epigenetically silenced resulting in a deficit of the FMR1 gene product, FMRP. This results in fragile X Syndrome (FXS), the most common heritable cause of intellectual disability and autism. The diagnosis and study of these disorders is challenging, in part because the detection of alleles with large repeat numbers has, until recently, been either time-consuming or unreliable. This problem is compounded by the mosaicism for repeat length and/or DNA methylation that is frequently seen in PM and FM carriers. Furthermore, since AGG interruptions in the repeat tract affect the risk that a FM allele will be maternally transmitted, the ability to accurately detect these interruptions in female PM carriers is an additional challenge that must be met. This review will discuss some of the pros and cons of some recently described assays for these disorders, including those that detect FMRP levels directly, as well as emerging technologies that promise to improve the diagnosis of these conditions and to be useful in both basic and translational research settings.
Conflict of interest statement
Conflict of Interest: The authors have no conflict of interest
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
