

An Overview of Achalasia and Its Subtypes
- PMID: 28867969
- PMCID: PMC5572971
An Overview of Achalasia and Its Subtypes
Abstract
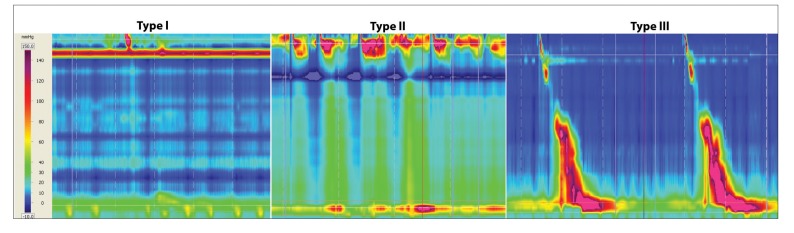
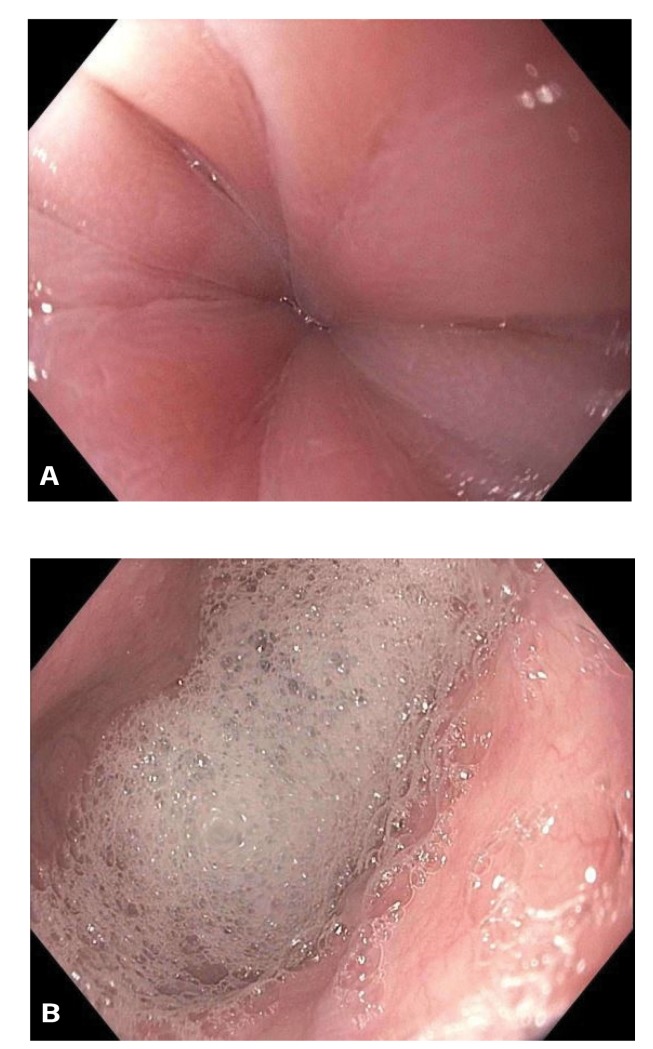
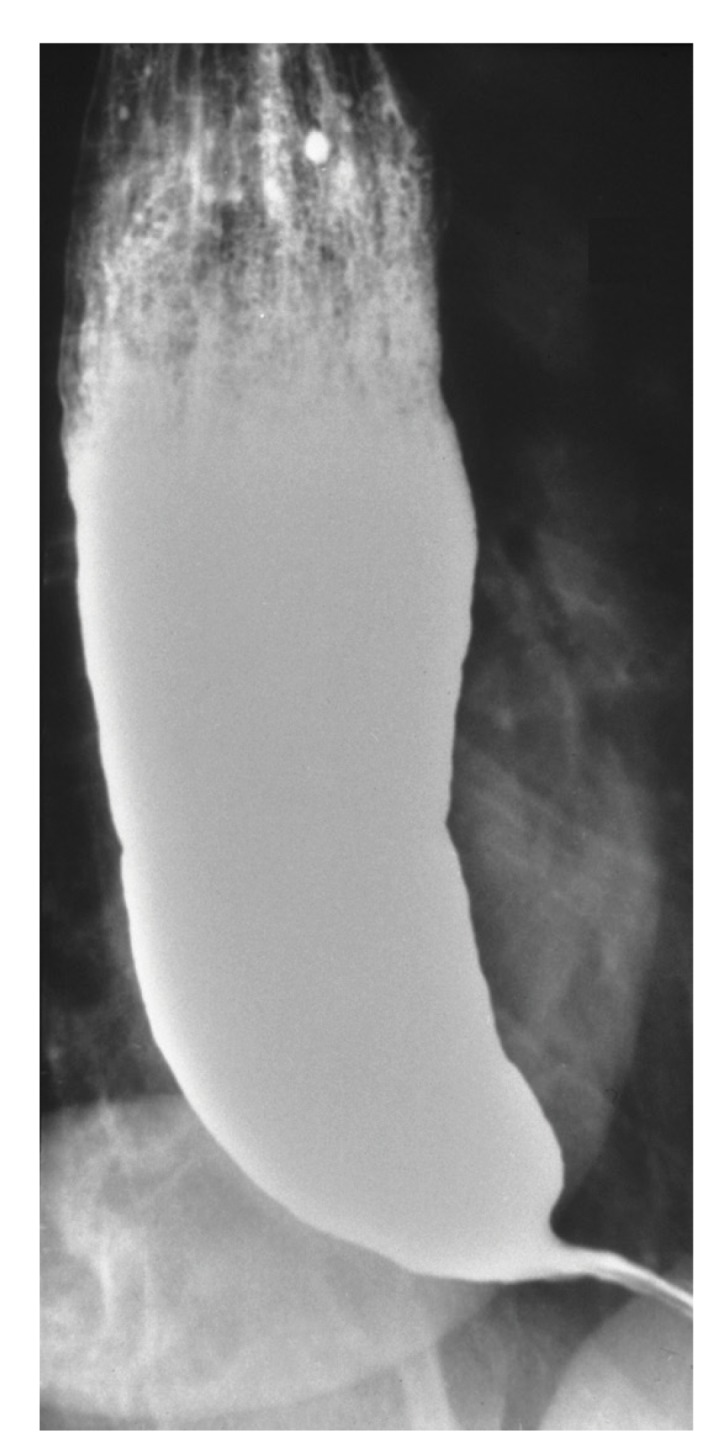
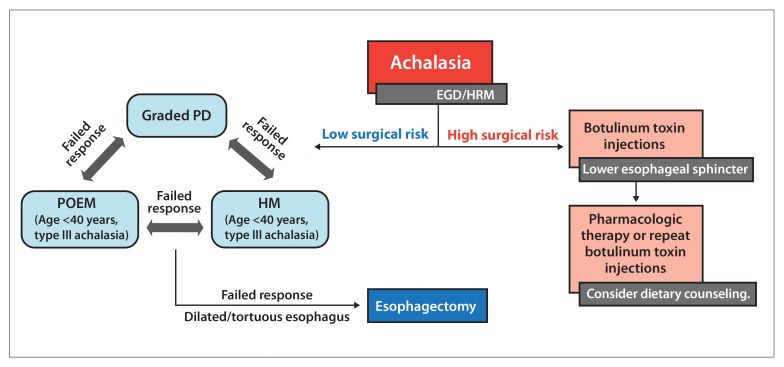
Achalasia is one of the most studied esophageal motility disorders. However, the pathophysiology and reasons that patients develop achalasia are still unclear. Patients often present with dysphagia to solids and liquids, regurgitation, and varying degrees of weight loss. There is significant latency prior to diagnosis, which can have nutritional implications. The diagnosis is suspected based on clinical history and confirmed by esophageal high-resolution manometry testing. Esophagogastroduodenoscopy is necessary to rule out potential malignancy that can mimic achalasia. Recent data presented in abstract form suggest that patients with type II achalasia may be most likely, and patients with type III achalasia may be least likely, to report weight loss compared to patients with type I achalasia. Although achalasia cannot be permanently cured, palliation of symptoms is possible in over 90% of patients with the treatment modalities currently available (pneumatic dilation, Heller myotomy, or peroral endoscopic myotomy). This article reviews the clinical presentation, diagnosis, and management options in patients with achalasia, as well as potential insights into histopathologic differences and nutritional implications of the subtypes of achalasia.
Keywords: Achalasia; histopathology; nutrition; weight loss.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures
References
-
- Farrukh A, DeCaestecker J, Mayberry JF. An epidemiological study of achalasia among the South Asian population of Leicester, 1986-2005. Dysphagia. 2008;23(2):161–164. - PubMed
-
- Birgisson S, Richter JE. Achalasia in Iceland, 1952-2002: an epidemiologic study. Dig Dis Sci. 2007;52(8):1855–1860. - PubMed
-
- Sadowski DC, Ackah F, Jiang B, Svenson LW. Achalasia: incidence, prevalence and survival. A population-based study. Neurogastroenterol Motil. 2010;22(9):e256–e261. - PubMed
-
- Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management of achalasia. Am J Gastroenterol. 2013;108(8):1238–1249. - PubMed
LinkOut - more resources
Full Text Sources