

New insights into the vitamin D requirements during pregnancy
- PMID: 28868163
- PMCID: PMC5573964
- DOI: 10.1038/boneres.2017.30
New insights into the vitamin D requirements during pregnancy
Abstract
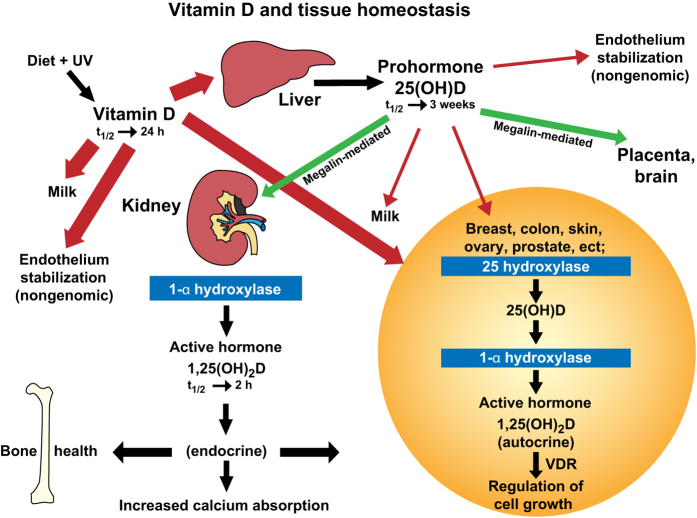
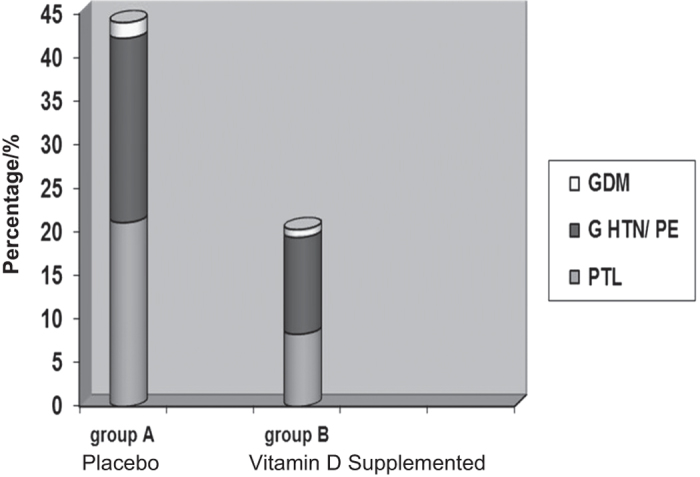
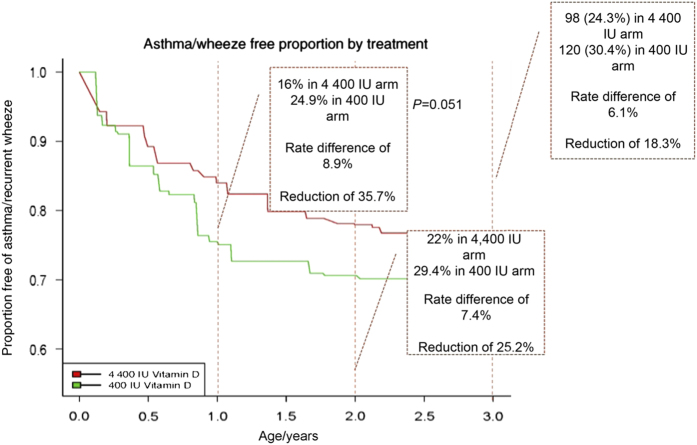
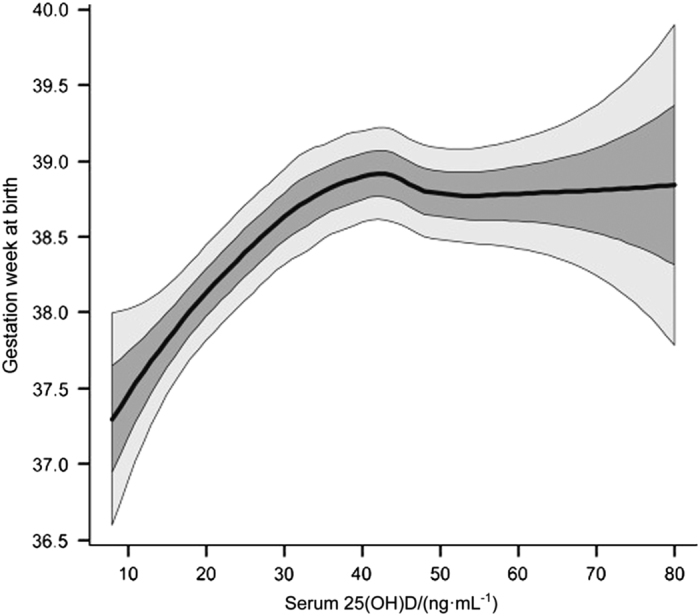
Pregnancy represents a dynamic period with physical and physiological changes in both the mother and her developing fetus. The dramatic 2-3 fold increase in the active hormone 1,25(OH)2D concentrations during the early weeks of pregnancy despite minimal increased calcium demands during that time of gestation and which are sustained throughout pregnancy in both the mother and fetus suggests an immunomodulatory role in preventing fetal rejection by the mother. While there have been numerous observational studies that support the premise of vitamin D's role in maintaining maternal and fetal well-being, until recently, there have been few randomized clinical trials with vitamin D supplementation. One has to exhibit caution, however, even with RCTs, whose results can be problematic when analyzed on an intent-to-treat basis and when there is high non-adherence to protocol (as if often the case), thereby diluting the potential good or harm of a given treatment at higher doses. As such, a biomarker of a drug or in this case "vitamin" or pre-prohormone is better served. For these reasons, the effect of vitamin D therapies using the biomarker circulating 25(OH)D is a far better indicator of true "effect." When pregnancy outcomes are analyzed using the biomarker 25(OH)D instead of treatment dose, there are notable differences in maternal and fetal outcomes across diverse racial/ethnic groups, with improved health in those women who attain a circulating 25(OH)D concentration of at least 100 nmol·L-1 (40 ng·mL-1). Because an important issue is the timing or initiation of vitamin D treatment/supplementation, and given the potential effect of vitamin D on placental gene expression and its effects on inflammation within the placenta, it appears crucial to start vitamin D treatment before placentation (and trophoblast invasion); however, this question remains unanswered. Additional work is needed to decipher the vitamin D requirements of pregnant women and the optimal timing of supplementation, taking into account a variety of lifestyles, body types, baseline vitamin D status, and maternal and fetal vitamin D receptor (VDR) and vitamin D binding protein (VDBP) genotypes. Determining the role of vitamin D in nonclassical, immune pathways continues to be a challenge that once answered will substantiate recommendations and public health policies.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Ross AC, Manson JE, Abrams SA et al. The 2011 Dietary Reference Intakes for Calcium and Vitamin D: what dietetics practitioners need to know. J Am Diet Assoc 2011; 111: 524–527. - PubMed
-
- World Health Organisation. Vitamin D Supplementation in Infants. Geneva: World Health Organisation. 2014.
-
- Camargo CA Jr, Ingham T, Wickens K et al. Cord-Blood 25-Hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthama. Pediatrics 2011; 127: e180–e187. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
