

Renin-angiotensin blockade in heart failure with preserved ejection fraction: a systematic review and meta-analysis
- PMID: 28869332
- PMCID: PMC5695183
- DOI: 10.1002/ehf2.12204
Renin-angiotensin blockade in heart failure with preserved ejection fraction: a systematic review and meta-analysis
Abstract
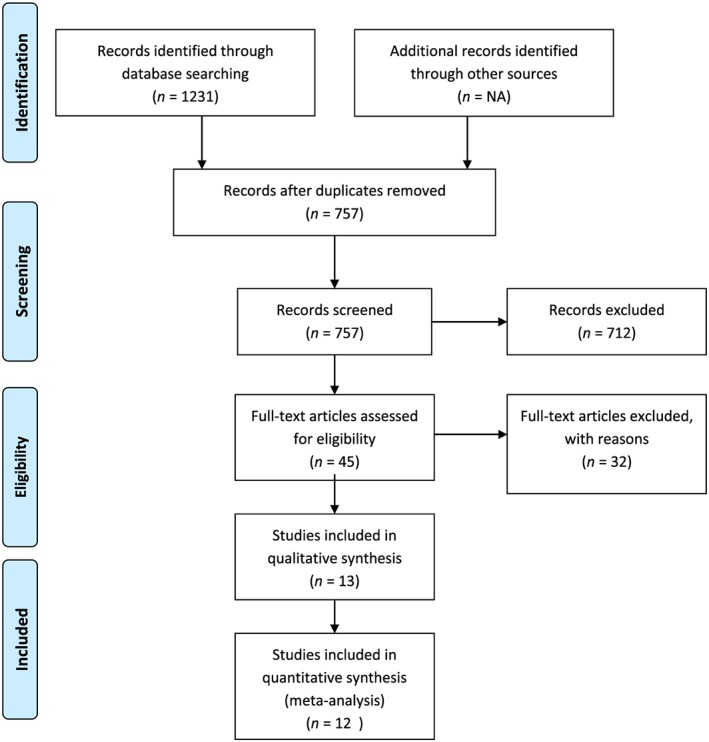
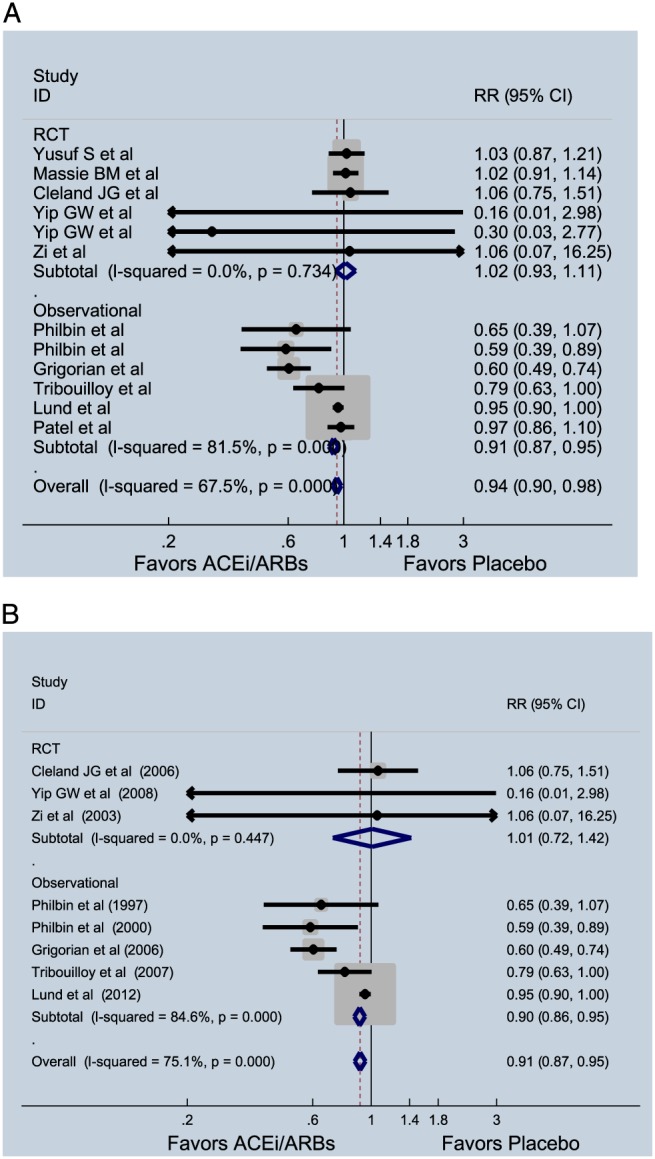
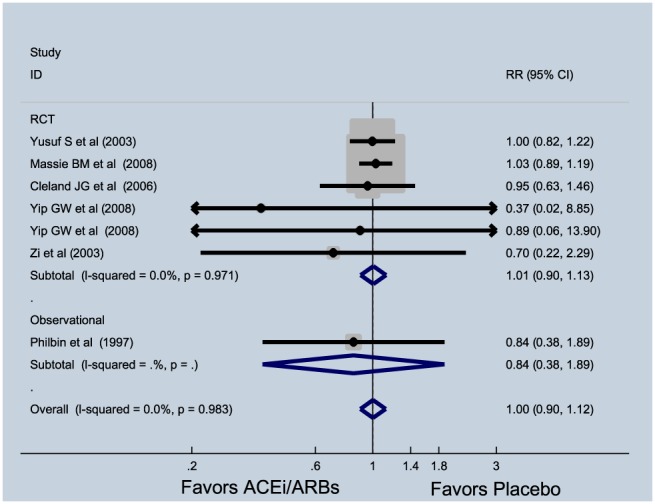
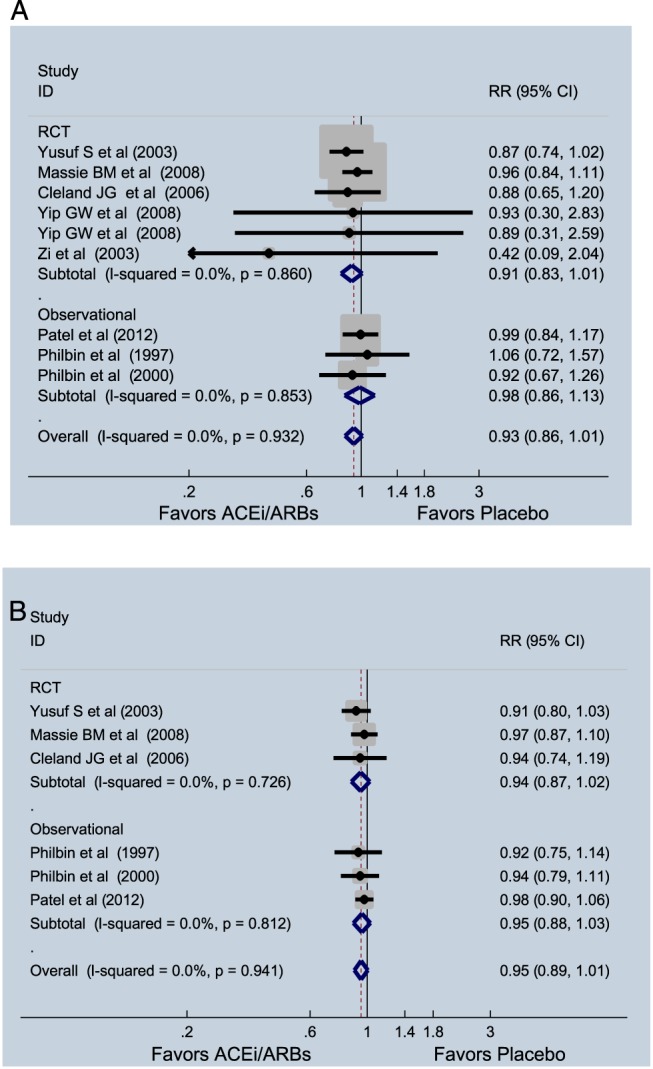
Studies with angiotensin-converting enzyme inhibitors (ACE-Is) and angiotensin receptor blockers (ARBs) in patients with heart failure with preserved ejection fraction (HFpEF) have yielded inconsistent results. To conduct a systematic review and meta-analysis of all evidence for ACE-I and ARBs in patients with HFpEF, we searched PubMed, Ovid SP, Embase, and Cochrane database to identify randomized trials and observational studies that compared ACE-I or ARBs against placebo or standard therapy in HFpEF patients. Random-effect models were used to pool the data, and I2 testing was performed to assess the heterogeneity of the included studies. A total of 13 studies (treatment arm = 8676 and control arm = 8608) were analysed. Pooled analysis of randomized trials for ACE-I and ARBs (n = 6) did not show any effect on all-cause mortality [relative risk (RR) = 1.02, 95% confidence interval (CI) = 0.93-1.11, P = 0.68, I2 = 0%], while results from observational studies showed a significant improvement (RR = 0.91, 95% CI = 0.87-0.95, P = 0.005, I2 = 81.5%). In pooled analyses of all studies, ACE-I showed a reduction of all-cause mortality (RR = 0.91, 95% CI = 0.87-0.95, P = 0.01). There was no reduction in cardiovascular mortality seen, but in pooled analysis of randomized trials, there was a trend towards reduced HF hospitalization risk (RR = 0.91, 95% CI = 0.83-1.01, I2 = 0%, P = 0.074). These data suggest that ACE-I and ARBs may have a role in improving outcomes of patients with HFpEF, underscoring the need for future research with careful patient selection, and trial design and conduct.
Keywords: Angiotensin receptor blockers; Angiotensin-converting enzyme inhibitors; Heart failure; Preserved ejection fraction; Renin-angiotensin system.
© 2017 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Figures
References
-
- Owan TE, Redfield MM. Epidemiology of diastolic heart failure. Prog Cardiovasc Dis 2005; 47: 320–332. - PubMed
-
- Owan TE, Do H, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006; 355: 251–259. - PubMed
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of heart failure with preserved ejection in a population‐based study. N Engl J Med 2006; 355: 260–269. - PubMed
-
- Yusuf S, Pfeffer MA, Swedberg K, Granger CB, Held P, McMurray JJ, Michelson EL, Olofsson B, Ostergren J, CHARM Investigators and Committees . Effects of candesartan in patients with chronic heart failure and preserved left‐ventricular ejection fraction: the CHARM‐Preserved Trial. Lancet 2003; 362: 777–781. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
