

Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials
- PMID: 28869989
- PMCID: PMC5734053
- DOI: 10.7326/M16-2586
Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials
Abstract
Background: The ERSPC (European Randomized Study of Screening for Prostate Cancer) found that screening reduced prostate cancer mortality, but the PLCO (Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial) found no reduction.
Objective: To evaluate whether effects of screening on prostate cancer mortality relative to no screening differed between the ERSPC and PLCO.
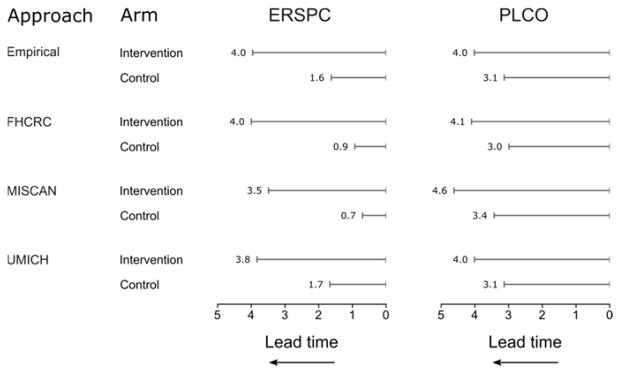
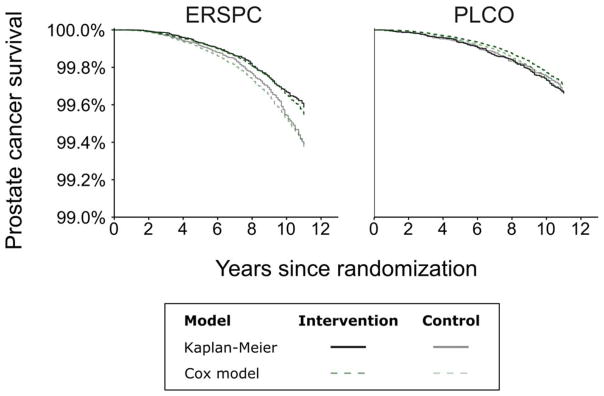
Design: Cox regression of prostate cancer death in each trial group, adjusted for age and trial. Extended analyses accounted for increased incidence due to screening and diagnostic work-up in each group via mean lead times (MLTs), which were estimated empirically and using analytic or microsimulation models.
Setting: Randomized controlled trials in Europe and the United States.
Participants: Men aged 55 to 69 (ERSPC) or 55 to 74 (PLCO) years at randomization.
Intervention: Prostate cancer screening.
Measurements: Prostate cancer incidence and survival from randomization; prostate cancer incidence in the United States before screening began.
Results: Estimated MLTs were similar in the ERSPC and PLCO intervention groups but were longer in the PLCO control group than the ERSPC control group. Extended analyses found no evidence that effects of screening differed between trials (P = 0.37 to 0.47 [range across MLT estimation approaches]) but strong evidence that benefit increased with MLT (P = 0.0027 to 0.0032). Screening was estimated to confer a 7% to 9% reduction in the risk for prostate cancer death per year of MLT. This translated into estimates of 25% to 31% and 27% to 32% lower risk for prostate cancer death with screening as performed in the ERSPC and PLCO intervention groups, respectively, compared with no screening.
Limitation: The MLT is a simple metric of screening and diagnostic work-up.
Conclusion: After differences in implementation and settings are accounted for, the ERSPC and PLCO provide compatible evidence that screening reduces prostate cancer mortality.
Primary funding source: National Cancer Institute.
Figures
Comment in
-
Prostate Cancer Screening: Time to Question How to Optimize the Ratio of Benefits and Harms.Ann Intern Med. 2017 Oct 3;167(7):509-510. doi: 10.7326/M17-2012. Epub 2017 Sep 5. Ann Intern Med. 2017. PMID: 28869975 No abstract available.
-
Pooled RCTs: Reanalysis accounting for screening intensity suggests that screening reduces prostate cancer mortality.Ann Intern Med. 2018 Jan 16;168(2):JC5. doi: 10.7326/ACPJC-2018-168-2-005. Ann Intern Med. 2018. PMID: 29335717 No abstract available.
-
Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials.Ann Intern Med. 2018 Apr 17;168(8):606. doi: 10.7326/L17-0733. Ann Intern Med. 2018. PMID: 29677257 No abstract available.
-
Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials.Ann Intern Med. 2018 Apr 17;168(8):607-608. doi: 10.7326/L17-0734. Ann Intern Med. 2018. PMID: 29677258 No abstract available.
-
Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials.Ann Intern Med. 2018 Apr 17;168(8):605-606. doi: 10.7326/L17-0735. Ann Intern Med. 2018. PMID: 29677259 No abstract available.
-
Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials.Ann Intern Med. 2018 Apr 17;168(8):606-607. doi: 10.7326/L17-0736. Ann Intern Med. 2018. PMID: 29677260 No abstract available.
-
Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials.Ann Intern Med. 2018 Apr 17;168(8):608. doi: 10.7326/L17-0737. Ann Intern Med. 2018. PMID: 29677261 No abstract available.
-
Reconciling the Effects of Screening on Prostate Cancer Mortality in the ERSPC and PLCO Trials.Ann Intern Med. 2018 Apr 17;168(8):608-609. doi: 10.7326/L17-0738. Ann Intern Med. 2018. PMID: 29677262 No abstract available.
Summary for patients in
-
Different Effects of Screening on Prostate Cancer Death in Two Trials.Ann Intern Med. 2017 Oct 3;167(7). doi: 10.7326/P17-9043. Epub 2017 Sep 5. Ann Intern Med. 2017. PMID: 28869990 No abstract available.
References
-
- Moyer VA Force USPST. Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;157(2):120–34. - PubMed
-
- Jemal A, Fedewa SA, Ma J, Siegel R, Lin CC, Brawley O, et al. Prostate Cancer Incidence and PSA Testing Patterns in Relation to USPSTF Screening Recommendations. JAMA. 2015;314(19):2054–61. - PubMed
-
- Jemal A, Ma J, Siegel R, Fedewa S, Brawley O, Ward EM. Prostate Cancer Incidence Rates 2 Years After the US Preventive Services Task Force Recommendations Against Screening. JAMA Oncol. 2016;2(12):1657–60. - PubMed
-
- Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, et al. Screening and prostate-cancer mortality in a randomized European study. New England Journal of Medicine. 2009;360(13):1320–8. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical