

Progression of arterial stiffness is associated with changes in bone mineral markers in advanced CKD
- PMID: 28870151
- PMCID: PMC5584006
- DOI: 10.1186/s12882-017-0705-4
Progression of arterial stiffness is associated with changes in bone mineral markers in advanced CKD
Abstract
Background: Arterial stiffness is an independent predictor of all-cause and cardiovascular mortality in patients with chronic kidney disease (CKD). There are limited prospective data however on progression of arterial stiffness in CKD, including evaluating associations with bone mineral markers such as fibroblast growth factor 23 (FGF23) and soluble α-klotho (sKl).
Methods: In this prospective, single-center, observational study, arterial stiffness [measured by pulse wave velocity (PWV)] and hormones influencing mineral homeostasis, including serum FGF23 and sKl, were compared between non-dialysis CKD stages 4/5 and healthy controls at baseline and 12 months (12 m). Abdominal aortic calcification (AAC) was quantitated using lateral lumbar radiography at baseline.
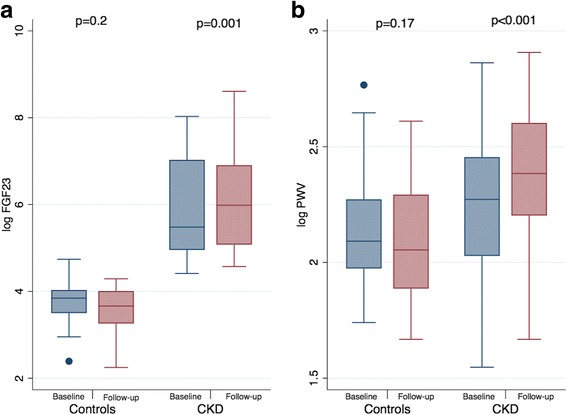
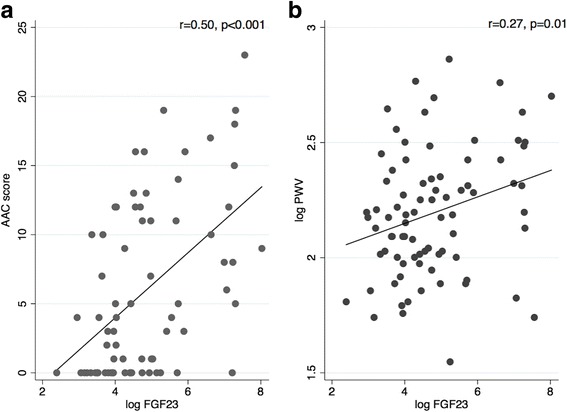
Results: Forty patients with CKD [mean estimated glomerular filtration rate (eGFR) 19.5 ± 6.7 mL/min/1.73m2] and 42 controls (mean eGFR 88.6 ± 12.9 mL/min/1.73m2) completed follow-up. There were no differences in age, gender and body mass index between groups. A significant increase in FGF23 [240.6 (141.9-1129.8) to 396.8 (160.3-997.7) pg/mL, p = 0.001] was observed in the CKD group but serum phosphate, corrected calcium, parathyroid hormone and sKl did not change significantly over 12 m. At baseline, CKD subjects had higher AAC prevalence [83.8% versus (vs.) 43.6%, p = 0.002] and higher aortic PWV [9.7(7.6-11.7) vs. 8.1 (7.2-9.7) m/s, p = 0.047] compared to controls. At 12 m, aortic PWV increased by 1.3 m/s (95% confidence interval, 0.56 to 2.08, p < 0.001) in the CKD cohort, with 30% of subjects showing progression from normal aortic elasticity to stiffening (PWV > 10 m/s). Serum FGF23 was associated with AAC, abnormal PWV and progression of PWV at 12 m.
Conclusions: Arterial stiffness and serum FGF23, both of which are associated with increased cardiovascular risk, increased over one year in individuals with CKD. Additionally, a significant association was found between serum FGF23 and arterial calcification and stiffness. Larger clinical studies and further experimental work are warranted to delineate the temporal relationship as well as the pathological mechanisms linking FGF23 and vascular disease.
Keywords: Aortic calcification; Arterial stiffness; Chronic kidney disease; Fibroblast growth factor 23; Soluble klotho.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Metro South Health Human Research Ethics Committee (HREC 2012/480). Written informed consent was obtained from all participants before commencement of baseline visit for this study.
Consent for publication
Not applicable.
Competing interest
Associate Professor Carmel Hawley has received research funding from Baxter Healthcare Pty Ltd., Shire Pty. Limited and Fresenius Medical Care. She has received travel grants from Amgen Australia. Professor David Johnson is a consultant for Baxter Healthcare Pty Ltd. and has previously received research funds from this company. He has also received speakers’ honoraria and research grants from Fresenius Medical Care and is a recipient of a National Health and Medical Council Practitioner Fellowship. Associate Professor Isbel has received research funding from Baxter Healthcare Pty Ltd., Roche Pharmaceuticals and Amgen in the form of peer-reviewed grants. She has also received travel grants from Shire Australia, Alexion Pharmaceuticals and Pfizer. Dr. Rathika Krishnasamy and Dr. Sven-Jean Tan have received speaking honoraria from Shire Australia. Associate Professor Tony Stanton has acted as a consultant to Medtronic and Novartis Pharmaceuticals. David Mudge has received travel grants, consultancy fees and speakers’ honoraria from Baxter Healthcare, Amgen and Alexion. Dr. Sven-Jean Tan is a current recipient of the Australian National Health and Medical Research Council (NHMRC) Postgraduate Research Scholarship. Associate Professor Nigel Toussaint has received research funding and speaking honoraria from Shire, Sanofi and Amgen Australia. The remaining authors have no competing financial interests to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
FGF23 is independently associated with vascular calcification but not bone mineral density in patients at various CKD stages.Osteoporos Int. 2012 Jul;23(7):2017-25. doi: 10.1007/s00198-011-1838-0. Epub 2011 Nov 23. Osteoporos Int. 2012. PMID: 22109743
-
Secreted Klotho and FGF23 in chronic kidney disease Stage 1 to 5: a sequence suggested from a cross-sectional study.Nephrol Dial Transplant. 2013 Feb;28(2):352-9. doi: 10.1093/ndt/gfs460. Epub 2012 Nov 4. Nephrol Dial Transplant. 2013. PMID: 23129826
-
Association of serum adiponectin concentration with aortic arterial stiffness in chronic kidney disease: from the KNOW-CKD study.Clin Exp Nephrol. 2017 Aug;21(4):608-616. doi: 10.1007/s10157-016-1322-4. Epub 2016 Aug 11. Clin Exp Nephrol. 2017. PMID: 27514393
-
Arterial Stiffness and Decline in Kidney Function.Clin J Am Soc Nephrol. 2015 Dec 7;10(12):2190-7. doi: 10.2215/CJN.03000315. Epub 2015 Nov 12. Clin J Am Soc Nephrol. 2015. PMID: 26563380 Free PMC article. Review.
-
FGF23 and Klotho in chronic kidney disease.Curr Opin Nephrol Hypertens. 2013 Jul;22(4):397-404. doi: 10.1097/MNH.0b013e32836213ee. Curr Opin Nephrol Hypertens. 2013. PMID: 23666415 Review.
Cited by
-
Correlation between soluble klotho and chronic kidney disease-mineral and bone disorder in chronic kidney disease: a meta-analysis.Sci Rep. 2024 Feb 23;14(1):4477. doi: 10.1038/s41598-024-54812-4. Sci Rep. 2024. PMID: 38396063 Free PMC article.
-
Chronic Kidney Disease and Pulse Wave Velocity: A Narrative Review.Int J Hypertens. 2019 Feb 17;2019:9189362. doi: 10.1155/2019/9189362. eCollection 2019. Int J Hypertens. 2019. PMID: 30906591 Free PMC article. Review.
-
Disability of Dialysis Patients and the Condition of Blood Vessels.J Clin Med. 2020 Jun 10;9(6):1806. doi: 10.3390/jcm9061806. J Clin Med. 2020. PMID: 32531965 Free PMC article.
-
Relationship between Residual Urine Output and Type of Dialysis with FGF23 Levels.J Clin Med. 2022 Dec 28;12(1):222. doi: 10.3390/jcm12010222. J Clin Med. 2022. PMID: 36615023 Free PMC article.
-
Association of serum Klotho and fibroblast growth factor-23 levels with vascular calcification severity in patients with chronic kidney disease: an observational cohort study.Int Urol Nephrol. 2025 Aug;57(8):2711-2719. doi: 10.1007/s11255-025-04475-5. Epub 2025 Apr 1. Int Urol Nephrol. 2025. PMID: 40167982 Free PMC article.
References
-
- Karras A, Haymann JP, Bozec E, Metzger M, Jacquot C, Maruani G, Houillier P, Froissart M, Stengel B, Guardiola P, et al. Large artery stiffening and remodeling are independently associated with all-cause mortality and cardiovascular events in chronic kidney disease. Hypertension. 2012;60(6):1451–1457. doi: 10.1161/HYPERTENSIONAHA.112.197210. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
