

Post-resuscitation arterial oxygen and carbon dioxide and outcomes after out-of-hospital cardiac arrest
- PMID: 28870720
- PMCID: PMC5660655
- DOI: 10.1016/j.resuscitation.2017.08.244
Post-resuscitation arterial oxygen and carbon dioxide and outcomes after out-of-hospital cardiac arrest
Abstract
Objective: To determine if arterial oxygen and carbon dioxide abnormalities in the first 24h after return of spontaneous circulation (ROSC) are associated with increased mortality in adult out-of-hospital cardiac arrest (OHCA).
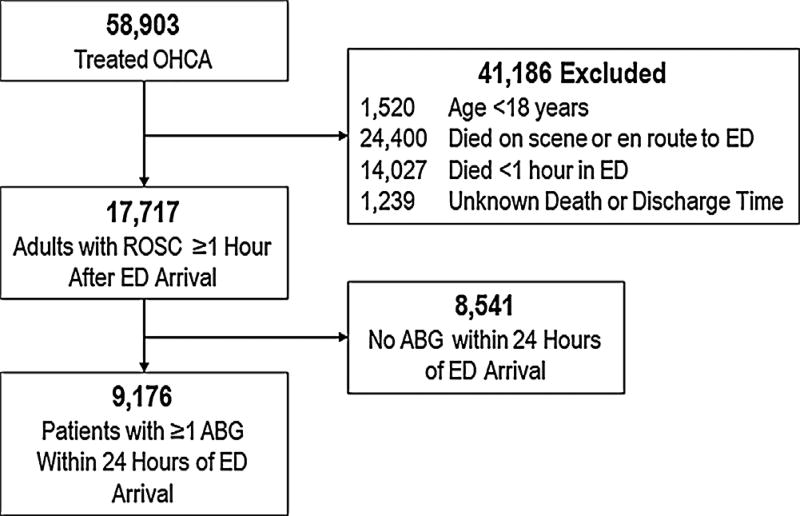
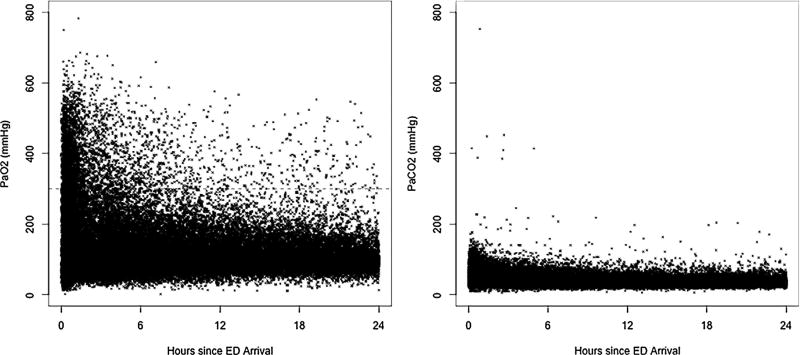
Methods: We used data from the Resuscitation Outcomes Consortium (ROC), including adult OHCA with sustained ROSC ≥1h after Emergency Department arrival and at least one arterial blood gas (ABG) measurement. Among ABGs measured during the first 24h of hospitalization, we identified the presence of hyperoxemia (PaO2≥300mmHg), hypoxemia (PaO2<60mmHg), hypercarbia (PaCO2>50mmHg) and hypocarbia (PaCO2<30mmHg). We evaluated the associations between oxygen and carbon dioxide abnormalities and hospital mortality, adjusting for confounders.
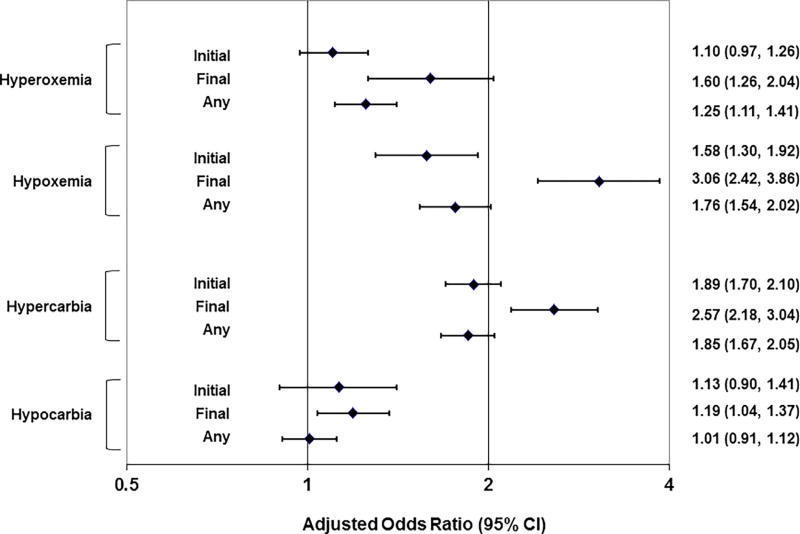
Results: Among 9186 OHCA included in the analysis, hospital mortality was 67.3%. Hyperoxemia, hypoxemia, hypercarbia, and hypocarbia occurred in 26.5%, 19.0%, 51.0% and 30.6%, respectively. Initial hyperoxemia only was not associated with hospital mortality (adjusted OR 1.10; 95% CI: 0.97-1.26). However, final and any hyperoxemia (1.25; 1.11-1.41) were associated with increased hospital mortality. Initial (1.58; 1.30-1.92), final (3.06; 2.42-3.86) and any (1.76; 1.54-2.02) hypoxemia (PaO2<60mmHg) were associated with increased hospital mortality. Initial (1.89; 1.70-2.10); final (2.57; 2.18-3.04) and any (1.85; 1.67-2.05) hypercarbia (PaCO2>50mmHg) were associated with increased hospital mortality. Initial (1.13; 0.90-1.41), final (1.19; 1.04-1.37) and any (1.01; 0.91-1.12) hypocarbia (PaCO2<30mmHg) were not associated with hospital mortality.
Conclusions: In the first 24h after ROSC, abnormal post-arrest oxygen and carbon dioxide tensions are associated with increased out of-hospital cardiac arrest mortality.
Keywords: Cardiopulmonary arrest; Hypercarbia; Hyperoxemia; Hypocarbia; Hypoxemia; Post-arrest care.
Copyright © 2017 Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Comment in
-
Cerebral resuscitation: Shifting away from the basics.Resuscitation. 2017 Dec;121:e11. doi: 10.1016/j.resuscitation.2017.09.028. Epub 2017 Sep 28. Resuscitation. 2017. PMID: 28965929 No abstract available.
-
Reply to: "Cerebral resuscitation: Shifting away from the basics" (Letter to editor on post-resuscitation arterial oxygen and carbon dioxide and outcomes after out-of-hospital cardiac arrest).Resuscitation. 2017 Dec;121:e13. doi: 10.1016/j.resuscitation.2017.10.014. Epub 2017 Oct 23. Resuscitation. 2017. PMID: 29074399 No abstract available.
References
-
- Idris AH, Staples ED, O’Brien DJ, et al. Effect of ventilation on acid-base balance and oxygenation in low blood-flow states. Crit Care Med. 1994;22(11):1827–34. - PubMed
-
- Angelos MG, Yeh ST, Aune SE. Post-cardiac arrest hyperoxia and mitochondrial function. Resuscitation. 2011;82(Suppl. 2):S48–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
