

Severe Tuberculosis in Humans Correlates Best with Neutrophil Abundance and Lymphocyte Deficiency and Does Not Correlate with Antigen-Specific CD4 T-Cell Response
- PMID: 28871253
- PMCID: PMC5566990
- DOI: 10.3389/fimmu.2017.00963
Severe Tuberculosis in Humans Correlates Best with Neutrophil Abundance and Lymphocyte Deficiency and Does Not Correlate with Antigen-Specific CD4 T-Cell Response
Abstract
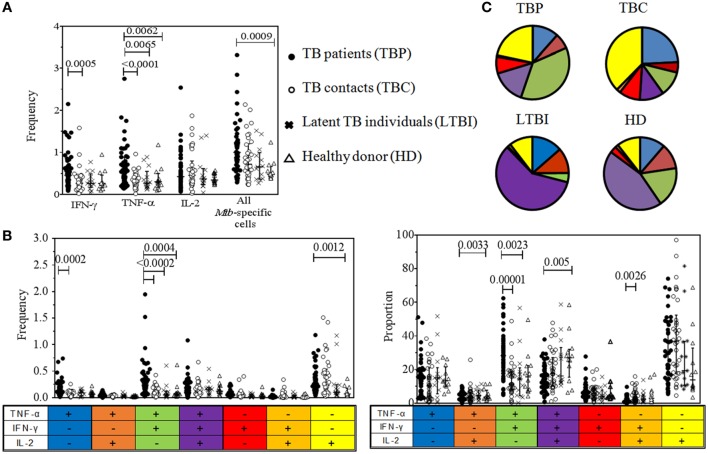
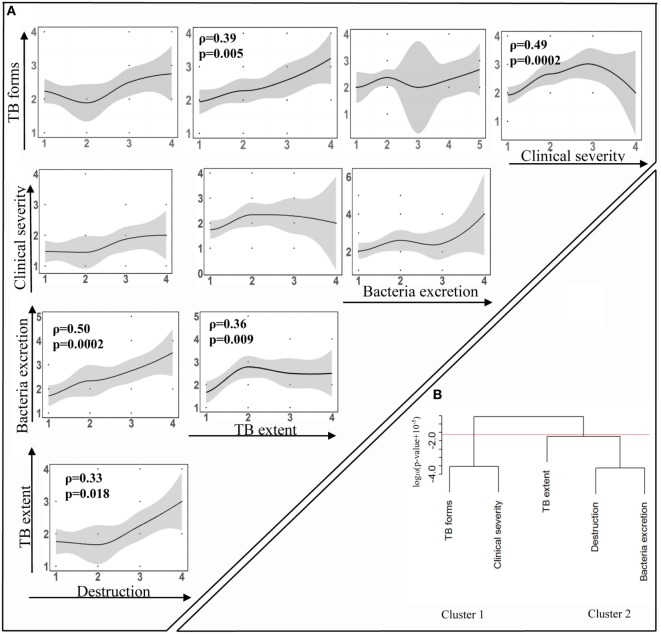
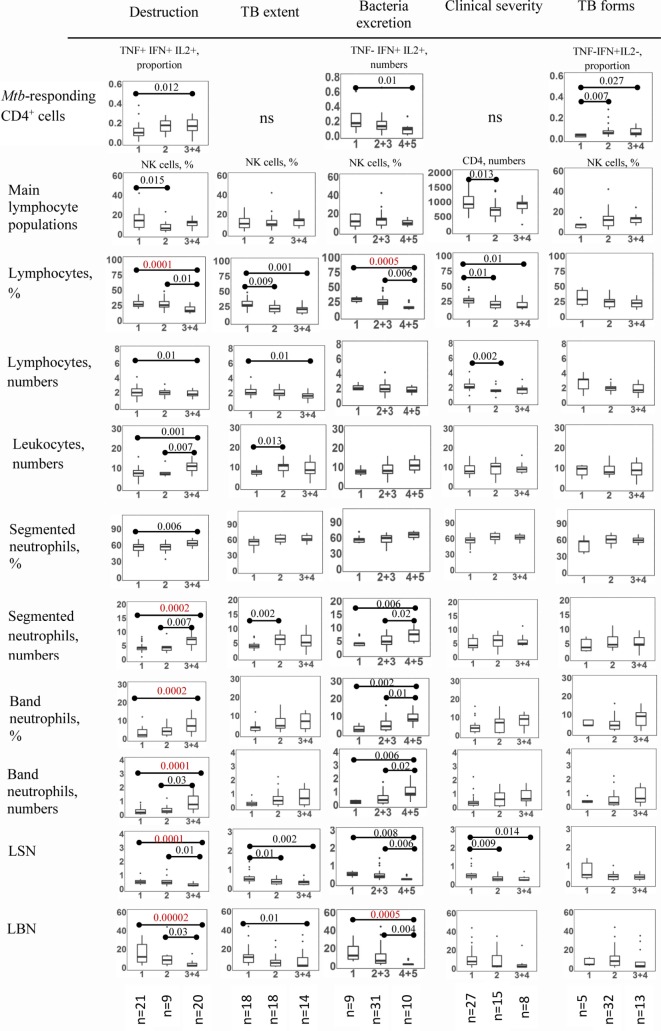
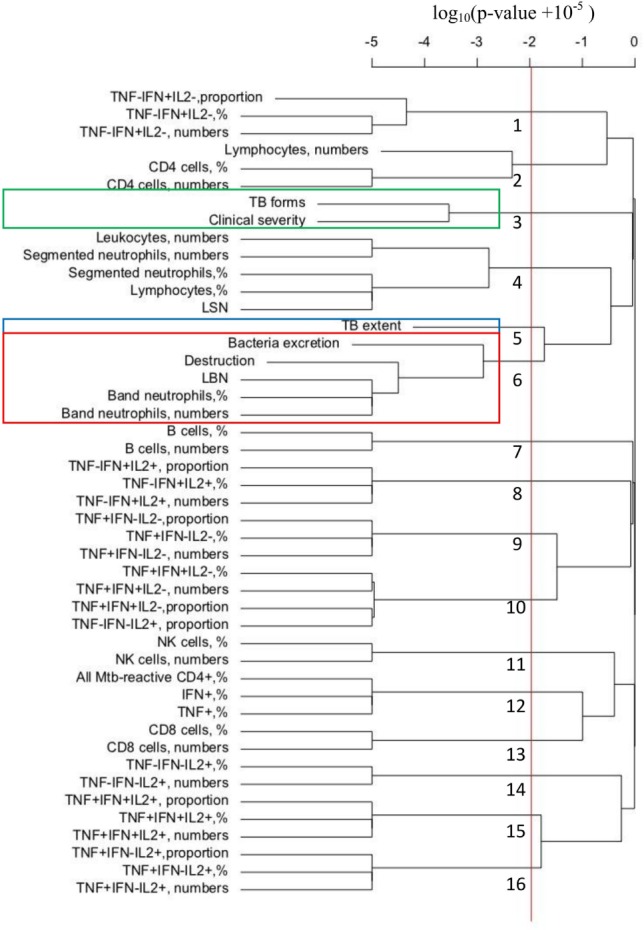
It is generally thought that Mycobacterium tuberculosis (Mtb)-specific CD4+ Th1 cells producing IFN-γ are essential for protection against tuberculosis (TB). In some studies, protection has recently been associated with polyfunctional subpopulation of Mtb-specific Th1 cells, i.e., with cells able to simultaneously secrete several type 1 cytokines. However, the role for Mtb-specific Th1 cells and their polyfunctional subpopulations during established TB disease is not fully defined. Pulmonary TB is characterized by a great variability of disease manifestations. To address the role for Mtb-specific Th1 responses during TB, we investigated how Th1 and other immune cells correlated with particular TB manifestations, such as the degree of pulmonary destruction, TB extent, the level of bacteria excretion, clinical disease severity, clinical TB forms, and "Timika X-ray score," an integrative parameter of pulmonary TB pathology. In comparison with healthy Mtb-exposed controls, TB patients (TBP) did not exhibit deficiency in Mtb-specific cytokine-producing CD4+ cells circulating in the blood and differed by a polyfunctional profile of these cells, which was biased toward the accumulation of bifunctional TNF-α+IFN-γ+IL-2- lymphocytes. Importantly, however, severity of different TB manifestations was not associated with Mtb-specific cytokine-producing cells or their polyfunctional profile. In contrast, several TB manifestations were strongly correlated with leukocyte numbers, the percent or the absolute number of lymphocytes, segmented or band neutrophils. In multiple alternative statistical analyses, band neutrophils appeared as the strongest positive correlate of pulmonary destruction, bacteria excretion, and "Timika X-ray score." In contrast, clinical TB severity was primarily and inversely correlated with the number of lymphocytes in the blood. The results suggest that: (i) different TB manifestations may be driven by distinct mechanisms; (ii) quantitative parameters and polyfunctional profile of circulating Mtb-specific CD4+ cells play a minor role in determining TB severity; and (iii) general shifts in production/removal of granulocytic and lymphocytic lineages represent an important factor of TB pathogenesis. Mechanisms leading to these shifts and their specific role during TB are yet to be determined but are likely to involve changes in human hematopoietic system.
Keywords: Th1 cells; band neutrophils; neutrophils; polyfunctional lymphocytes; pulmonary destruction; tuberculosis.
Figures
References
-
- WHO. Global Tuberculosis Report 2016. Geneva: World Health Organization; (2016). Available from: http://apps.who.int/iris/bitstream/10665/250441/1/9789241565394-eng.pdf
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials