

Syphilis Infection Differentially Regulates the Phenotype and Function of γδ T Cells in HIV-1-Infected Patients Depends on the HIV-1 Disease Stage
- PMID: 28871259
- PMCID: PMC5566620
- DOI: 10.3389/fimmu.2017.00991
Syphilis Infection Differentially Regulates the Phenotype and Function of γδ T Cells in HIV-1-Infected Patients Depends on the HIV-1 Disease Stage
Abstract
A rapidly escalating outbreak of syphilis infection has been affected men who have sex with men, particularly those with HIV-1 infection. γδ T cells are unconventional immune cells with two main subsets, Vδ1 T cells and Vδ2 T cells, which possess a combination of innate and adaptive immune features allowing them against HIV-1. However, whether syphilis infection affects the phenotype and function of γδ T cells in HIV-1-infected patients remains unclear, especially in acute HIV-1 infection (AHI). In this study, we enrolled 57 HIV-1-infected patients (24 with HIV-1 infection only and 33 coinfected with syphilis) from an acute HIV-1-infected cohort in Beijing (PRIMO). A comprehensive analysis of γδ T-cell phenotype and function was performed by flow cytometry. We found syphilis coinfection could reverse the imbalance of Vδ1/Vδ2 ratio in AHI. Syphilis infection results in decreased γδ T-cell activation in AHI, but increased γδ T-cell activation in chronic HIV-1 infection (CHI). Moreover, patients with CHI had larger numbers of IL-17-producing γδ T cells than those with AHI, regardless of syphilis status. Thus, syphilis affected the γδ T-cell immune response differently in patients depending on the stages of HIV-1 disease. In addition, the percentage of IL-17-producing γδ T cells was positively correlated with the percentage of neutrophils. These results suggest that the γδ T-cell/IL-17/neutrophil axis is involved in HIV-1 pathogenesis and disease progression. Taken together, our observations provide new insight into the roles of γδ T cells in immunopathogenesis of syphilis and HIV-1 coinfection, particularly during AHI, and our findings may be helpful for the prevention of syphilis and other sexually transmitted infections and highlight the great significance on the remedy of patients coinfected with HIV-1.
Keywords: IL-17; acute/chronic HIV-1 infection; innate immune response; syphilis; γδ T cells.
Figures
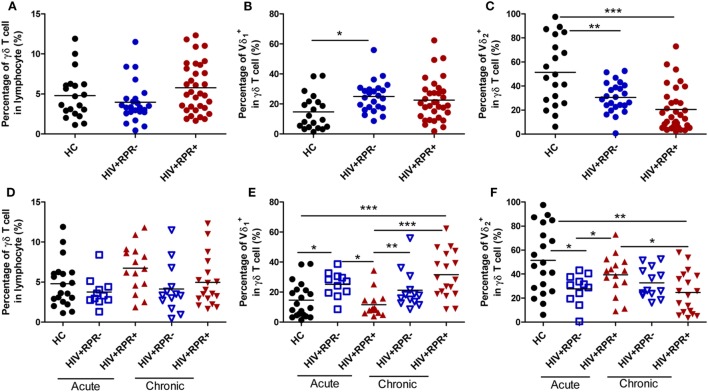
 ), and HIV+RPR+ (
), and HIV+RPR+ ( ) groups. Next, HIV+RPR− and HIV+RPR+ groups were subdivided according to the acute or chronic nature of their HIV-1 infection. The percentages of γδ T cells (D), Vδ1 T cells (E), and Vδ2 T cells (F) were compared among HIV+RPR− (
) groups. Next, HIV+RPR− and HIV+RPR+ groups were subdivided according to the acute or chronic nature of their HIV-1 infection. The percentages of γδ T cells (D), Vδ1 T cells (E), and Vδ2 T cells (F) were compared among HIV+RPR− ( ) and HIV+RPR+ (
) and HIV+RPR+ ( ) groups in acute HIV-1 infection and HIV+RPR− (
) groups in acute HIV-1 infection and HIV+RPR− ( ) and HIV+RPR+ (
) and HIV+RPR+ ( ) groups in chronic HIV-1 infection. The significance of differences was determined by calculating P values in Mann–Whitney tests and one-way ANOVA test. *P < 0.05, **P < 0.01, ***P < 0.001. HC, healthy controls; HIV+RPR+, patients coinfected with HIV-1 and syphilis; HIV+RPR−, patients infected with HIV-1 without syphilis.
) groups in chronic HIV-1 infection. The significance of differences was determined by calculating P values in Mann–Whitney tests and one-way ANOVA test. *P < 0.05, **P < 0.01, ***P < 0.001. HC, healthy controls; HIV+RPR+, patients coinfected with HIV-1 and syphilis; HIV+RPR−, patients infected with HIV-1 without syphilis.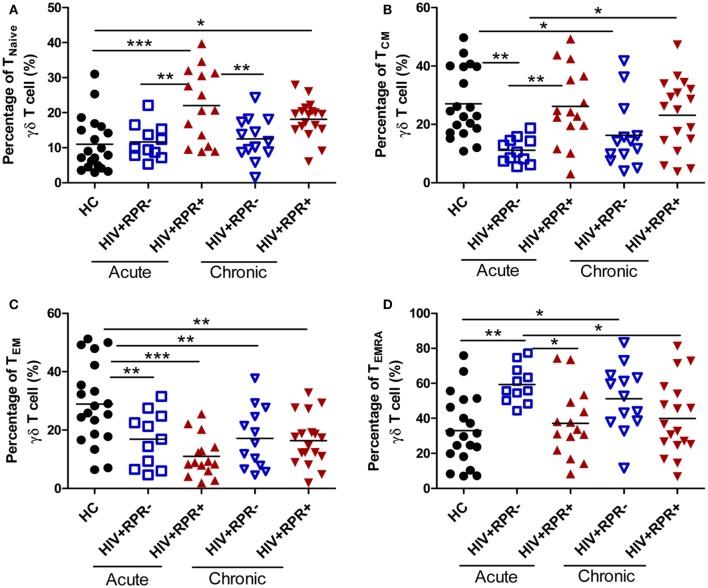 ), and HIV+RPR+ () groups in acute HIV-1-infected patients and HIV+RPR− () and HIV+RPR+ () groups in chronic HIV-1-infected patients. The significance of differences was assessed by calculating P values in Mann–Whitney tests. *P < 0.05, **P < 0.01, ***P < 0.001. RPR, rapid plasma reagin.
), and HIV+RPR+ () groups in acute HIV-1-infected patients and HIV+RPR− () and HIV+RPR+ () groups in chronic HIV-1-infected patients. The significance of differences was assessed by calculating P values in Mann–Whitney tests. *P < 0.05, **P < 0.01, ***P < 0.001. RPR, rapid plasma reagin.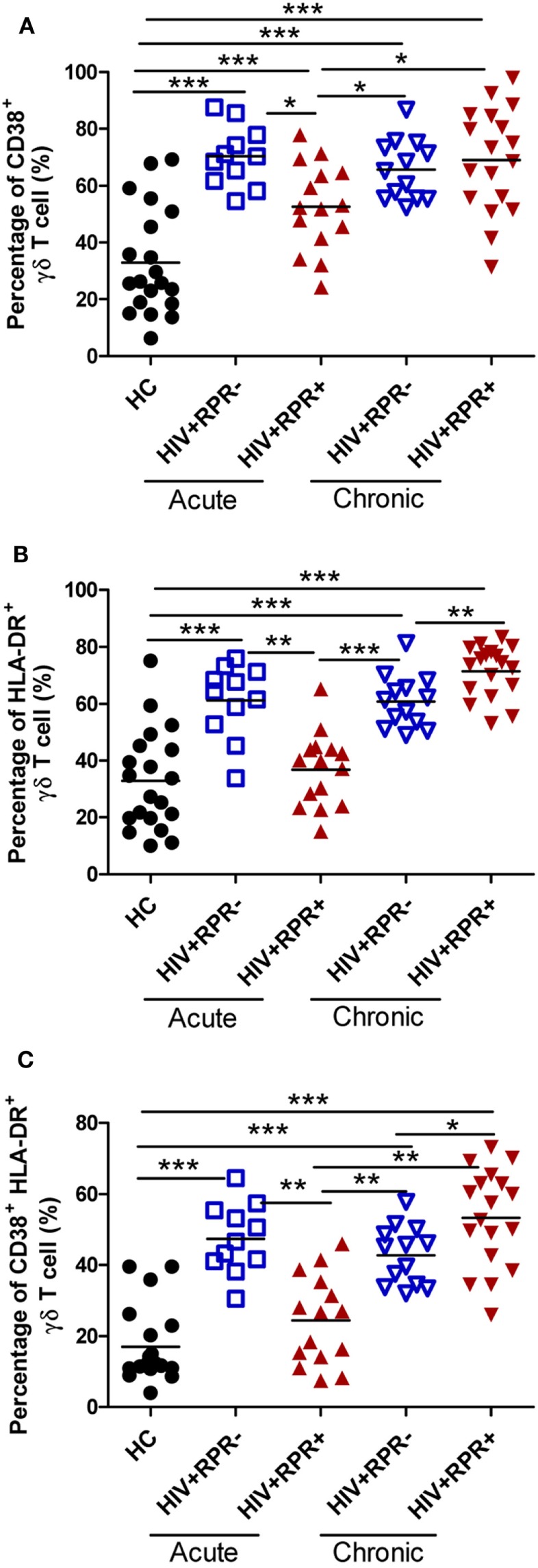 ), and HIV+RPR+ () groups in acute HIV-1-infected patients and HIV+RPR− () and HIV+RPR+ () groups in chronic HIV-1-infected patients. The significance of differences was determined by calculating P values in Mann–Whitney tests. *P < 0.05, **P < 0.01, ***P < 0.001. RPR, rapid plasma reagin.
), and HIV+RPR+ () groups in acute HIV-1-infected patients and HIV+RPR− () and HIV+RPR+ () groups in chronic HIV-1-infected patients. The significance of differences was determined by calculating P values in Mann–Whitney tests. *P < 0.05, **P < 0.01, ***P < 0.001. RPR, rapid plasma reagin.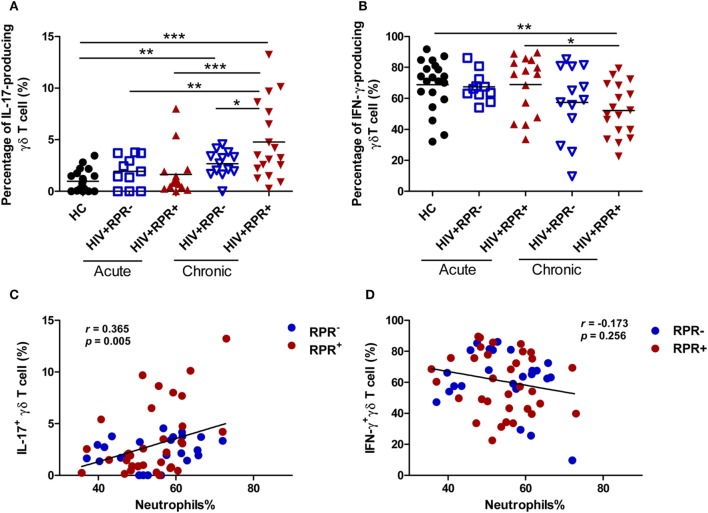 ) and HIV+RPR+ () groups in acute HIV-1-infected patients and HIV+RPR− () and HIV+RPR+ () groups in chronic HIV-1-infected patients. Correlations of the proportions of IL-17-producing γδ T cells (C) and IFN-γ-producing γδ T cells (D) with the percentage of neutrophils in HIV+RPR+ () and HIV+RPR− () groups were analyzed. The significance of differences was assessed by calculating P values in Mann–Whitney tests. Spearman’s rank correlation analysis was used to assess correlations. *P < 0.05, **P < 0.01, ***P < 0.001. RPR, rapid plasma reagin.
) and HIV+RPR+ () groups in acute HIV-1-infected patients and HIV+RPR− () and HIV+RPR+ () groups in chronic HIV-1-infected patients. Correlations of the proportions of IL-17-producing γδ T cells (C) and IFN-γ-producing γδ T cells (D) with the percentage of neutrophils in HIV+RPR+ () and HIV+RPR− () groups were analyzed. The significance of differences was assessed by calculating P values in Mann–Whitney tests. Spearman’s rank correlation analysis was used to assess correlations. *P < 0.05, **P < 0.01, ***P < 0.001. RPR, rapid plasma reagin.Similar articles
-
γδ T-cell responses during HIV infection and antiretroviral therapy.Clin Transl Immunology. 2019 Jul 17;8(7):e01069. doi: 10.1002/cti2.1069. eCollection 2019. Clin Transl Immunology. 2019. PMID: 31321033 Free PMC article. Review.
-
Inversed Ratio of CD39/CD73 Expression on γδ T Cells in HIV Versus Healthy Controls Correlates With Immune Activation and Disease Progression.Front Immunol. 2022 Apr 22;13:867167. doi: 10.3389/fimmu.2022.867167. eCollection 2022. Front Immunol. 2022. PMID: 35529864 Free PMC article.
-
Potential Role of Vδ2+ γδ T Cells in Regulation of Immune Activation in Primary HIV Infection.Front Immunol. 2017 Sep 25;8:1189. doi: 10.3389/fimmu.2017.01189. eCollection 2017. Front Immunol. 2017. PMID: 28993778 Free PMC article.
-
[Characteristics of γδ T cell subsets induced from peripheral blood mononuclear cells of HIV/AIDS patients in vitro].Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 2012 Mar;28(3):285-7. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 2012. PMID: 22394638 Chinese.
-
γδ T Cells in HIV Disease: Past, Present, and Future.Front Immunol. 2015 Jan 30;5:687. doi: 10.3389/fimmu.2014.00687. eCollection 2014. Front Immunol. 2015. PMID: 25688241 Free PMC article. Review.
Cited by
-
Syphilitic infection impairs immunity by inducing both apoptosis and pyroptosis of CD4+ and CD8+ T lymphocytes.Innate Immun. 2021 Jan;27(1):99-106. doi: 10.1177/1753425920952840. Epub 2020 Sep 1. Innate Immun. 2021. PMID: 32873094 Free PMC article.
-
Immunological Changes in Monocyte Subsets and Their Association With Foxp3+ Regulatory T Cells in HIV-1-Infected Individuals With Syphilis: A Brief Research Report.Front Immunol. 2019 Apr 9;10:714. doi: 10.3389/fimmu.2019.00714. eCollection 2019. Front Immunol. 2019. PMID: 31024549 Free PMC article.
-
Alterations of CCR2 and CX3CR1 on Three Monocyte Subsets During HIV-1/Treponema pallidum Coinfection.Front Med (Lausanne). 2020 Jun 18;7:272. doi: 10.3389/fmed.2020.00272. eCollection 2020. Front Med (Lausanne). 2020. PMID: 32626718 Free PMC article.
-
Dynamics and immunological signature of γδ T cells following antiretroviral therapy initiation in acute HIV-1 Infection.Front Immunol. 2025 May 8;16:1554916. doi: 10.3389/fimmu.2025.1554916. eCollection 2025. Front Immunol. 2025. PMID: 40406103 Free PMC article.
-
γδ T-cell responses during HIV infection and antiretroviral therapy.Clin Transl Immunology. 2019 Jul 17;8(7):e01069. doi: 10.1002/cti2.1069. eCollection 2019. Clin Transl Immunology. 2019. PMID: 31321033 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources