

Dermatomyositis and Immune-Mediated Necrotizing Myopathies: A Window on Autoimmunity and Cancer
- PMID: 28871260
- PMCID: PMC5566616
- DOI: 10.3389/fimmu.2017.00992
Dermatomyositis and Immune-Mediated Necrotizing Myopathies: A Window on Autoimmunity and Cancer
Abstract
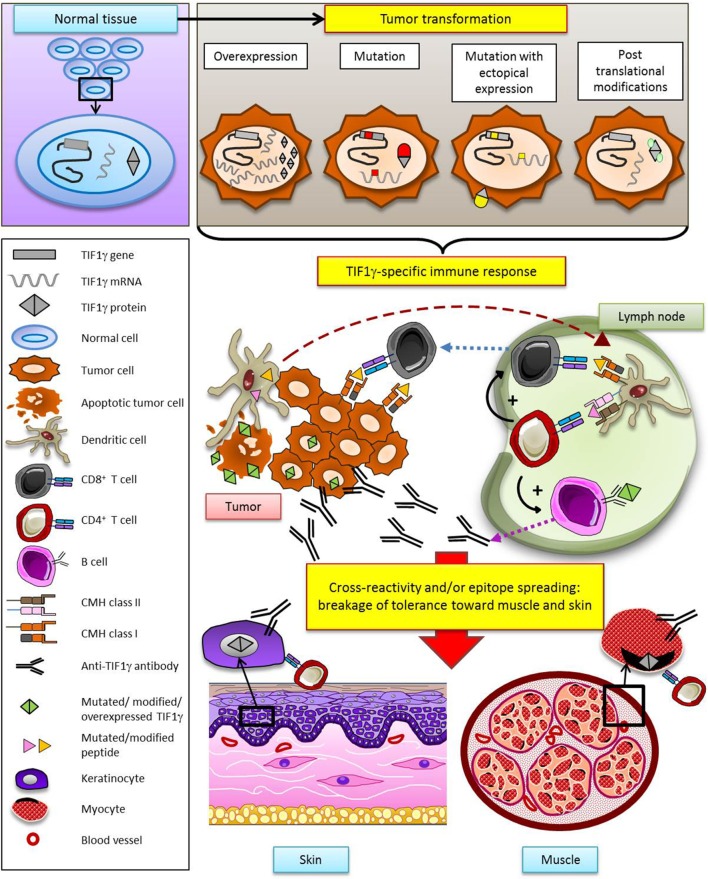
Autoimmune myopathies (myositides) are strongly associated with malignancy. The link between myositis and cancer, originally noticed by Bohan and Peter in their classification in 1975 (1), has been evidenced by large population-based cohort studies and a recent meta-analysis. The numerous reports of cases in which the clinical course of myositis reflects that of cancer and the short delay between myositis and cancer onset support the notion that myositis may be an authentic paraneoplastic disorder. Thus, cancer-associated myositis raises the question of cancer as a cause rather than a consequence of autoimmunity. Among myositides, dermatomyositis and more recently, although to a lesser extent, immune-mediated necrotizing myopathies are the most documented forms associated with cancer. Interestingly, the current diagnostic approach for myositis is based on the identification of specific antibodies where each antibody determines specific clinical features and outcomes. Recent findings have shown that the autoantibodies anti-TIF1γ, anti-NXP2 and anti-HMGCR are associated with cancers in the course of myositis. Herein, we highlight the fact that the targets of these three autoantibodies involve cellular pathways that intervene in tumor promotion and we discuss the role of cancer mutations as autoimmunity triggers in adult myositis.
Keywords: TIF1gamma; autoantibody; autoimmunity; cancer; myositis.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources