

Inversed-Planned Respiratory Phase Gating in Lung Conformal Radiation Therapy
- PMID: 28871981
- PMCID: PMC5656395
- DOI: 10.1016/j.ijrobp.2017.05.039
Inversed-Planned Respiratory Phase Gating in Lung Conformal Radiation Therapy
Abstract
Purpose: To assess whether the optimal gating window for each beam during lung radiation therapy with respiratory gating will be dependent on a variety of patient-specific factors, such as tumor size and location and the extent of relative tumor and organ motion.
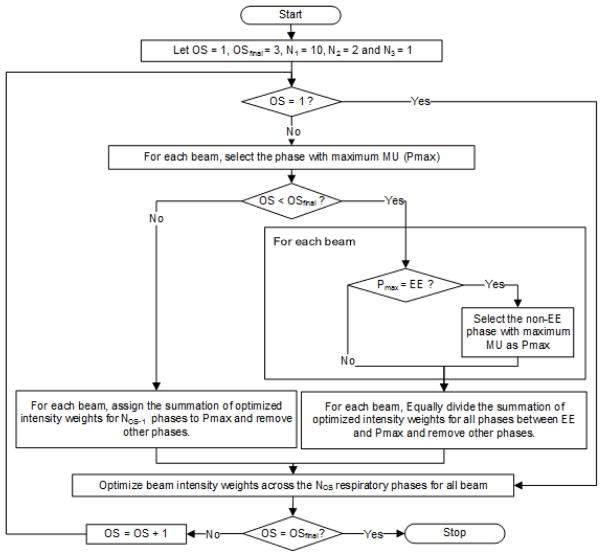
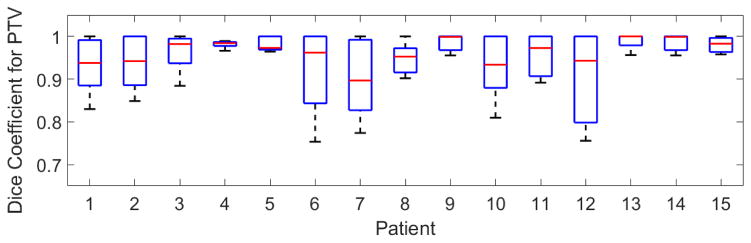
Methods and materials: To create optimal gating treatment plans, we started from an optimized clinical plan, created a plan per respiratory phase using the same beam arrangements, and used an inverse planning optimization approach to determine the optimal gating window for each beam and optimal beam weights (ie, monitor units). Two pieces of information were used for optimization: (1) the state of the anatomy at each phase, extracted from 4-dimensional computed tomography scans; and (2) the time spent in each state, estimated from a 2-minute monitoring of the patient's breathing motion. We retrospectively studied 15 lung cancer patients clinically treated by hypofractionated conformal radiation therapy, for whom 45 to 60 Gy was administered over 3 to 15 fractions using 7 to 13 beams. Mean gross tumor volume and respiratory-induced tumor motion were 82.5 cm3 and 1.0 cm, respectively.
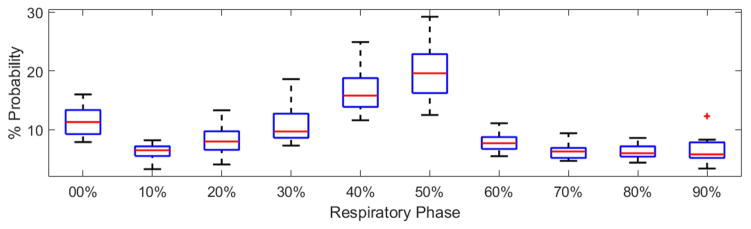
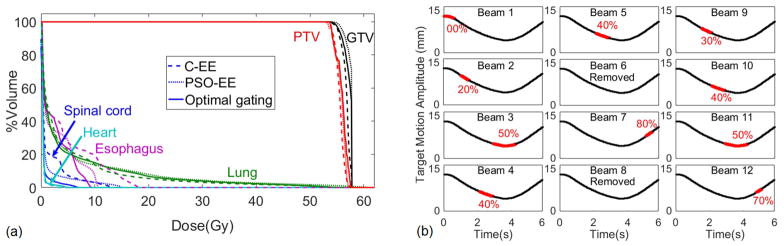
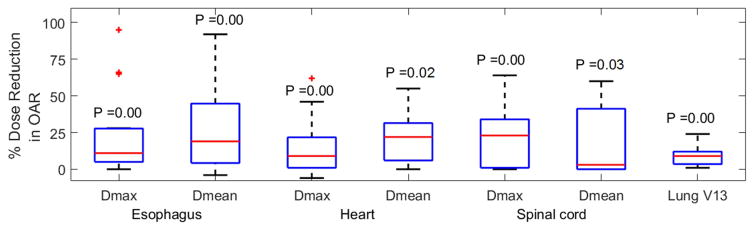
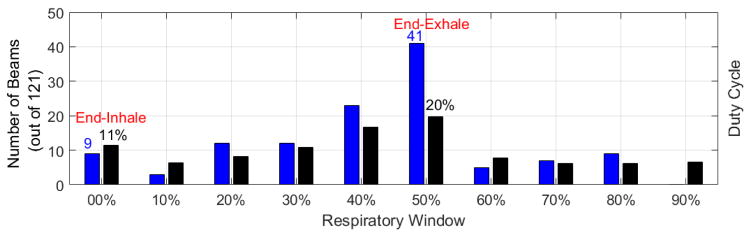
Results: Although patients spent most of their respiratory cycle in end-exhalation (EE), our optimal gating plans used EE for only 34% of the beams. Using optimal gating, maximum and mean doses to the esophagus, heart, and spinal cord were reduced by an average of 15% to 26%, and the beam-on times were reduced by an average of 23% compared with equivalent single-phase EE gated plans (P<.034, paired 2-tailed t test).
Conclusions: We introduce a personalized respiratory-gating technique in which inverse planning optimization is used to determine patient- and beam-specific gating phases toward enhancing dosimetric quality of radiation therapy treatment plans.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Nioutsikou E, Richard NSTJ, Bedford JL, Webb S. Quantifying the effect of respiratory motion on lung tumour dosimetry with the aid of a breathing phantom with deforming lungs. Phys Med Biol. 2006 Jul 21;51(14):3359–74. - PubMed
-
- Mutaf YD, Scicutella CJ, Michalski D, Fallon K, Brandner ED, Bednarz G, Huq MS. A simulation study of irregular respiratory motion and its dosimetric impact on lung tumors. Phys Med Biol. 2011 Feb 7;56(3):845–59. - PubMed
-
- Keall PJ, Mageras GS, Balter JM, Emery RS, Forster KM, Jiang SB, Kapatoes JM, Low DA, Murphy MJ, Murray BR, Ramsey CR, Van Herk MB, Vedam SS, Wong JW, Yorke E. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Med Phys. 2006 Oct;33(10):3874–900. - PubMed
-
- Schwarz M, Van der Geer J, Van Herk M, Lebesque JV, Mijnheer BJ, Damen EM. Impact of geometrical uncertainties on 3D CRT and IMRT dose distributions for lung cancer treatment. Int J Radiat Oncol Biol Phys. 2006 Jul 15;65(4):1260–9. - PubMed
-
- Timmerman RD, Hu C, Michalski J, Straube W, Galvin J, Johnstone D, Bradley J, Barriger R, Bezjak A, Videtic GM, Nedzi L, Werner-Wasik M, Chen Y, Komaki RU, Choy H. Long-term Results of RTOG 0236: A Phase II Trial of Stereotactic Body Radiation Therapy (SBRT) in the Treatment of Patients with Medically Inoperable Stage I Non-Small Cell Lung Cancer. International Journal of Radiation Oncology Biology Physics. 2014;90(1)
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
