

Prevalence and prognostic importance of precipitating factors leading to heart failure hospitalization: recurrent hospitalizations and mortality
- PMID: 28872259
- PMCID: PMC5826811
- DOI: 10.1002/ejhf.901
Prevalence and prognostic importance of precipitating factors leading to heart failure hospitalization: recurrent hospitalizations and mortality
Abstract
Aims: Hospitalizations for heart failure (HF) are common and are associated with significant morbidity, mortality and cost. However, precipitating factors leading to HF hospitalization and their importance with respect to subsequent outcomes are not well understood.
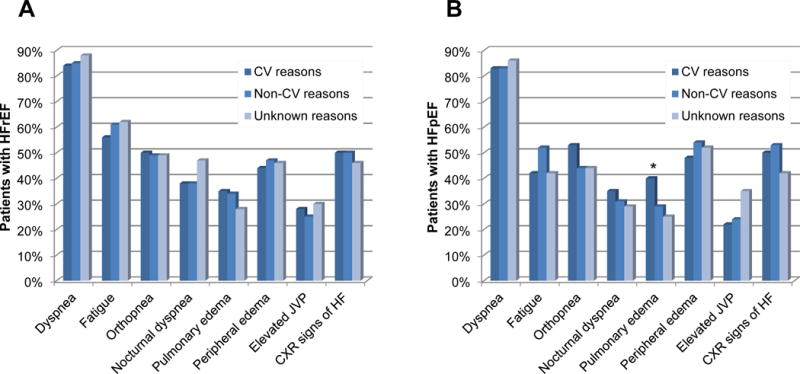
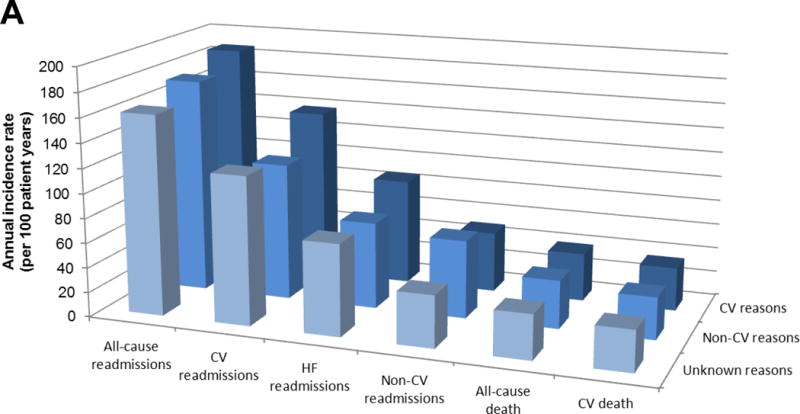
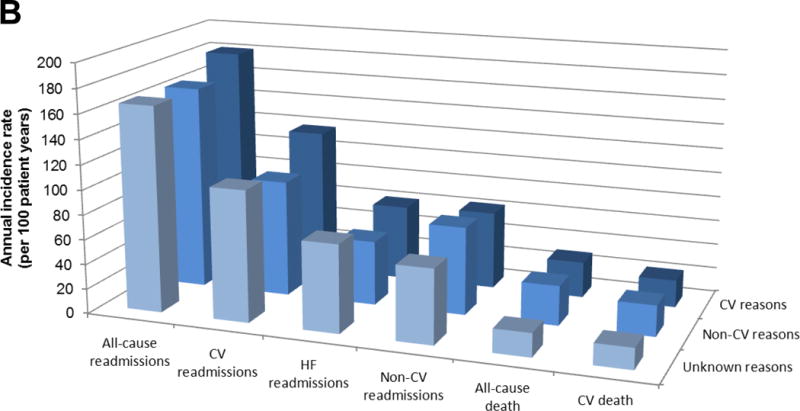
Methods and results: The symptoms and signs present at admission and investigator-identified factors thought to have contributed to the first adjudicated HF hospitalization in the Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) programme were prospectively collected and stratified by ejection fraction (EF). Potential precipitants were collected using a specifically designed case report form and categorized according to the presence of cardiovascular (CV), non-CV and unknown factors. Associations between these factors and subsequent rehospitalization and mortality rates were examined. Of 1668 patients who experienced HF hospitalization, 1152 had reduced EF (≤40%, HFrEF) and 516 had preserved EF (HFpEF). Overall, 54% had CV, 32% had non-CV and 14% had unknown factors thought to have precipitated HF, with similar proportions in the HFrEF and HFpEF groups. The most common precipitants were arrhythmia (15%), other non-CV factors (11%) and respiratory infection (10%). Subsequent CV readmission rates were highest in those whose initial HF hospitalization was precipitated by CV factors. However, mortality rates were similar among patients with any of the three categories of precipitating factors. Results were similar in HFrEF and HFpEF.
Conclusions: Among chronic HF patients hospitalized for decompensation, the investigator-reported precipitating factor was not associated with the subsequent mortality rate, but was associated with type of readmission: readmissions for CV reasons were more likely when the index precipitant was CV.
Keywords: Ejection fraction; Heart failure; Hospitalization; Precipitating factors; Prognosis.
© 2017 The Authors. European Journal of Heart Failure © 2017 European Society of Cardiology.
Conflict of interest statement
Dr. McMurray has nothing to disclose.
Figures
References
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Pina IL, Trogdon JG. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6:606–19. - PMC - PubMed
-
- Tsuyuki RT, McKelvie RS, Arnold JM, Avezum A, Jr, Barretto AC, Carvalho AC, Isaac DL, Kitching AD, Piegas LS, Teo KK, Yusuf S. Acute precipitants of congestive heart failure exacerbations. Arch Intern Med. 2001;161:2337–42. - PubMed
-
- Opasich C, Rapezzi C, Lucci D, Gorini M, Pozzar F, Zanelli E, Tavazzi L, Maggioni AP, Italian Network on Congestive Heart Failure I Precipitating factors and decision-making processes of short-term worsening heart failure despite “optimal” treatment (from the IN-CHF Registry) Am J Cardiol. 2001;88:382–7. - PubMed
-
- Fonarow GC, Abraham WT, Albert NM, Stough WG, Gheorghiade M, Greenberg BH, O’Connor CM, Pieper K, Sun JL, Yancy CW, Young JB, Investigators O-H and Hospitals Factors identified as precipitating hospital admissions for heart failure and clinical outcomes: findings from OPTIMIZE-HF. Arch Intern Med. 2008;168:847–54. - PubMed
-
- Kapoor JR, Kapoor R, Ju C, Heidenreich PA, Eapen ZJ, Hernandez AF, Butler J, Yancy CW, Fonarow GC. Precipitating Clinical Factors, Heart Failure Characterization, and Outcomes in Patients Hospitalized With Heart Failure With Reduced, Borderline, and Preserved Ejection Fraction. JACC Heart Fail. 2016;4:464–72. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
