

To err is human, to correct is public health: a systematic review examining poor quality testing and misdiagnosis of HIV status
- PMID: 28872271
- PMCID: PMC5625583
- DOI: 10.7448/IAS.20.7.21755
To err is human, to correct is public health: a systematic review examining poor quality testing and misdiagnosis of HIV status
Abstract
Introduction: In accordance with global testing and treatment targets, many countries are seeking ways to reach the "90-90-90" goals, starting with diagnosing 90% of all people with HIV. Quality HIV testing services are needed to enable people with HIV to be diagnosed and linked to treatment as early as possible. It is essential that opportunities to reach people with undiagnosed HIV are not missed, diagnoses are correct and HIV-negative individuals are not inadvertently initiated on life-long treatment. We conducted this systematic review to assess the magnitude of misdiagnosis and to describe poor HIV testing practices using rapid diagnostic tests.
Methods: We systematically searched peer-reviewed articles, abstracts and grey literature published from 1 January 1990 to 19 April 2017. Studies were included if they used at least two rapid diagnostic tests and reported on HIV misdiagnosis, factors related to potential misdiagnosis or described quality issues and errors related to HIV testing.
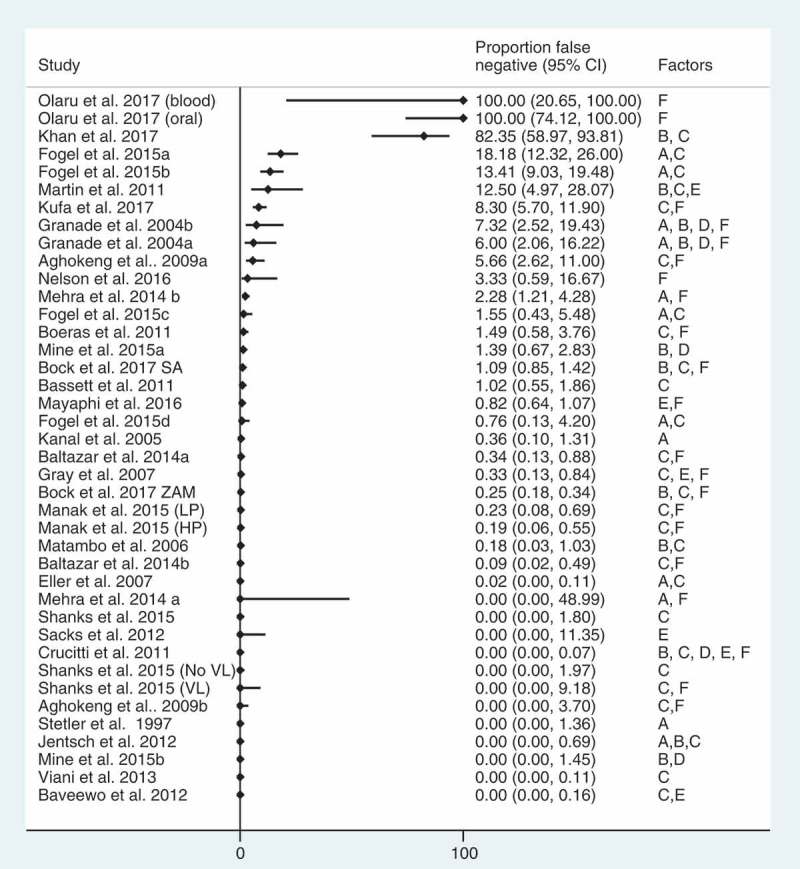
Results: Sixty-four studies were included in this review. A small proportion of false positive (median 3.1%, interquartile range (IQR): 0.4-5.2%) and false negative (median: 0.4%, IQR: 0-3.9%) diagnoses were identified. Suboptimal testing strategies were the most common factor in studies reporting misdiagnoses, particularly false positive diagnoses due to using a "tiebreaker" test to resolve discrepant test results. A substantial proportion of false negative diagnoses were related to retesting among people on antiretroviral therapy. Conclusions HIV testing errors and poor practices, particularly those resulting in false positive or false negative diagnoses, do occur but are preventable. Efforts to accelerate HIV diagnosis and linkage to treatment should be complemented by efforts to improve the quality of HIV testing services and strengthen the quality management systems, particularly the use of validated testing algorithms and strategies, retesting people diagnosed with HIV before initiating treatment and providing clear messages to people with HIV on treatment on the risk of a "false negative" test result.
Keywords: HIV; HIV testing; diagnostic error; false positive; healthcare; misclassification; misdiagnosis; patient safety.
Conflict of interest statement
The authors declare no completing interests. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions or policies of the institutions with which they are affiliated.
Figures


References
-
- WHO Towards universal access by 2010: how WHO is working with countries to scale-up HIV prevention, treatment, care and support. Geneva:World Health Organization;2006.
-
- WHO Factsheet to the WHO consolidated guidelines on HIV testing services. Geneva:World Health Organization;2015. - PubMed
-
- UNAIDS Get on the fast-track: the life cycle approach to HIV. Geneva:Joint United Nations Programme on HIV/AIDS;2016.
-
- Plate DK, Group, RHIVTEW . Evaluation and implementation of rapid HIV tests: the experience in 11 African countries. AIDS Res Hum Retroviruses. 2007;23(12):1491–98. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
