

Identification of misdiagnosed HIV clients in an Early Access to ART for All implementation study in Swaziland
- PMID: 28872273
- PMCID: PMC5625592
- DOI: 10.7448/IAS.20.7.21756
Identification of misdiagnosed HIV clients in an Early Access to ART for All implementation study in Swaziland
Abstract
Introduction: Rapid diagnostic testing has made HIV diagnosis and subsequent treatment more accessible. However, multiple factors, including improper implementation of testing strategies and clerical errors, have been reported to lead to HIV misdiagnosis. The World Health Organization has recommended HIV retesting prior to antiretroviral therapy (ART) initiation which has become pertinent with scaling up of Early Access to ART for All (EAAA). In this analysis, misdiagnosed clients are identified from a subgroup of clients enrolled in EAAA implementation study in Swaziland.
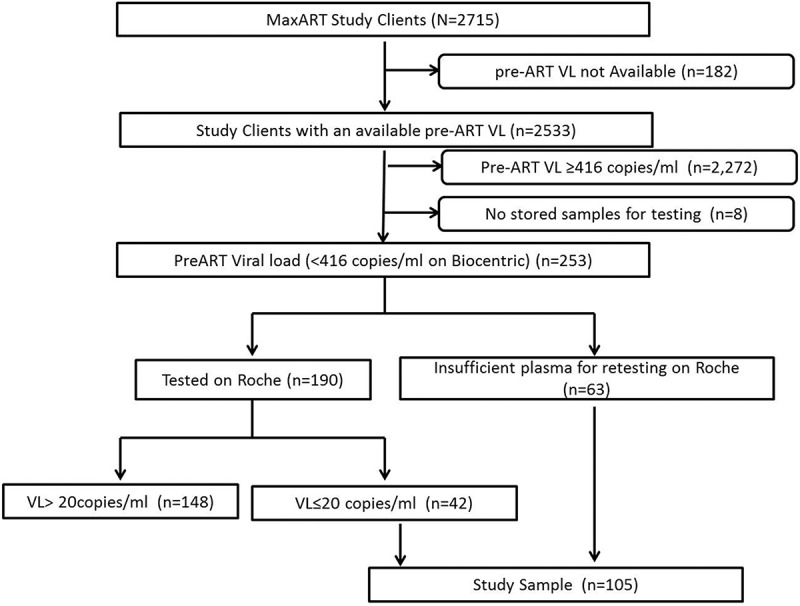
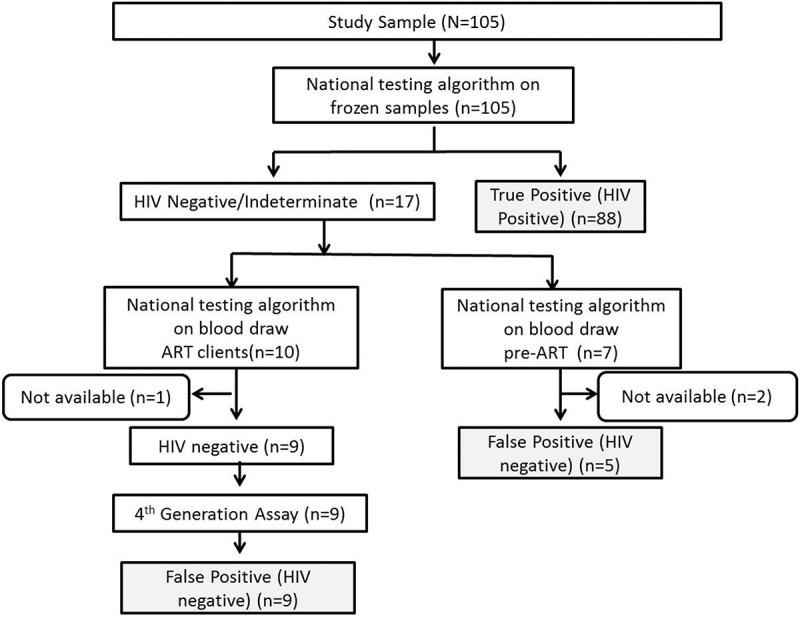
Methods: The subgroup to assess misdiagnosis was identified from enrolled EAAA study clients, who had an undetectable viral load prior to ART initiation between September 1, 2014 and May 31, 2016. One hundred and five of 2533 (4%) clients had an undetectable viral load prior to initiation to ART (pre-ART). The HIV status of clients was confirmed using the Determine HIV 1/2 and Uni-Gold HIV 1/2 rapid tests performed serially as recommended by the national testing algorithm. The status of clients on ART was additionally confirmed by fourth-generation HIV Ag/Ab combo tests, Architect and Genscreen Ultra.
Results: Fourteen of the 105 (13%) clients were false positive (HIV negative) on confirmation testing, of whom five (36%) were still in pre-ART care, while nine (64%) were in ART care. Overall, proportion of false positive was 0.6% (14/2533). The false-positive clients had a median CD4 of 791 cells/ml (interquartile range (IQR): 628, 967) compared to 549 cells/ml (IQR: 387, 791) for true positives (HIV positive) (p = 0.0081) and were nearly 20 years older (p = 0.0008).
Conclusions: Overall 0.6% of all enrolled EAAA clients were misdiagnosed, and 64% of misdiagnosed clients were initiated on ART. With adoption of EAAA guidelines by national governments, ART initiation regardless of immunological criteria, strengthening of proficiency testing and adoption of retesting prior to ART initiation would allow identification of misdiagnosed clients and further reduce potential of initiating misdiagnosed clients on ART.
Keywords: Early Access to ART for All; HIV false positive; HIV misdiagnosis; HIV testing; Swaziland; Universal test and treat; treatment for all.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- World Health Organization Service delivery approaches to HIV testing and counseling (HTC). Geneva: WHO, 2012.
-
- Johnson C, Fonner V, Sands A, Tsui S, Ford N, Wong V, et al. A report on the misdiagnosis of HIV status. Geneva: WHO, 2015.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
