

Relating gastric scintigraphy and symptoms to motility capsule transit and pressure findings in suspected gastroparesis
- PMID: 28872760
- PMCID: PMC6004323
- DOI: 10.1111/nmo.13196
Relating gastric scintigraphy and symptoms to motility capsule transit and pressure findings in suspected gastroparesis
Abstract
Background: Wireless motility capsule (WMC) findings are incompletely defined in suspected gastroparesis. We aimed to characterize regional WMC transit and contractility in relation to scintigraphy, etiology, and symptoms in patients undergoing gastric emptying testing.
Methods: A total of 209 patients with gastroparesis symptoms at NIDDK Gastroparesis Consortium centers underwent gastric scintigraphy and WMCs on separate days to measure regional transit and contractility. Validated questionnaires quantified symptoms.
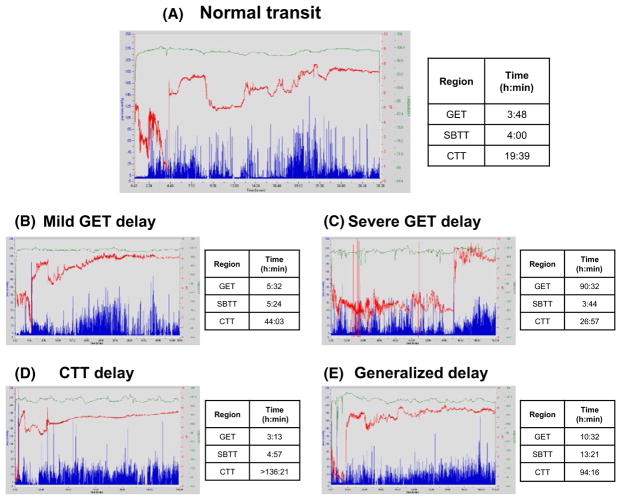
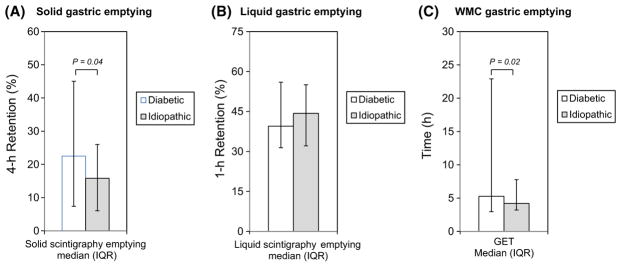
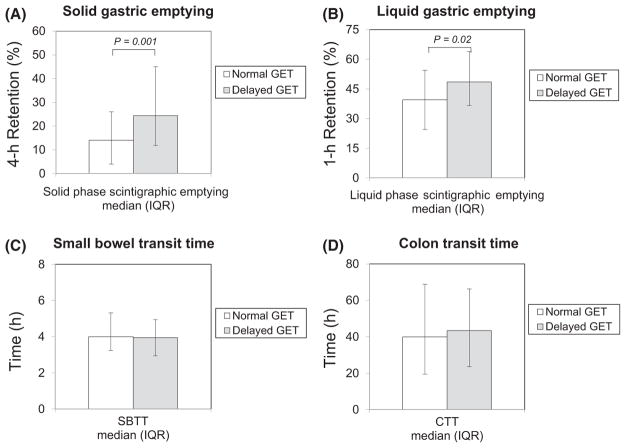
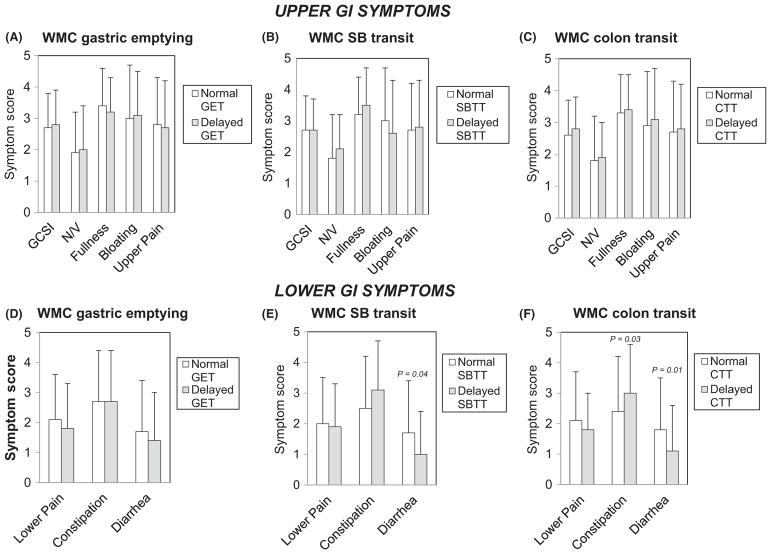
Key results: Solid scintigraphy and liquid scintigraphy were delayed in 68.8% and 34.8% of patients; WMC gastric emptying times (GET) were delayed in 40.3% and showed 52.8% agreement with scintigraphy; 15.5% and 33.5% had delayed small bowel (SBTT) and colon transit (CTT) times. Transit was delayed in ≥2 regions in 23.3%. Rapid transit was rarely observed. Diabetics had slower GET but more rapid SBTT versus idiopathics (P ≤ .02). GET delays related to greater scintigraphic retention, slower SBTT, and fewer gastric contractions (P ≤ .04). Overall gastroparesis symptoms and nausea/vomiting, early satiety/fullness, bloating/distention, and upper abdominal pain subscores showed no relation to WMC transit. Upper and lower abdominal pain scores (P ≤ .03) were greater with increased colon contractions. Constipation correlated with slower CTT and higher colon contractions (P = .03). Diarrhea scores were higher with delayed SBTT and CTT (P ≤ .04).
Conclusions & inferences: Wireless motility capsules define gastric emptying delays similar but not identical to scintigraphy that are more severe in diabetics and relate to reduced gastric contractility. Extragastric transit delays occur in >40% with suspected gastroparesis. Gastroparesis symptoms show little association with WMC profiles, although lower symptoms relate to small bowel or colon abnormalities.
Keywords: contractility; gastric emptying; scintigraphy; small bowel and colon transit.
© 2017 John Wiley & Sons Ltd.
Figures
References
-
- Hasler WL. Gastroparesis: pathogenesis, diagnosis and management. Nat Rev Gastroenterol Hepatol. 2011;8:438–453. - PubMed
-
- Abell TL, Camilleri M, Donohoe K, et al. Consensus recommendations for gastric emptying scintigraphy: a joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. Am J Gastroenterol. 2008;103:753–763. - PubMed
-
- Tougas G, Eaker EY, Abell TL, et al. Assessment of gastric emptying using a low fat meal: establishment of international control values. Am J Gastroenterol. 2000;95:1456–1462. - PubMed
-
- Kuo B, McCallum RW, Koch KL, et al. Comparison of gastric emptying of a nondigestible capsule to a radiolabelled meal in healthy and gastroparetic subjects. Aliment Pharmacol Ther. 2008;27:186–196. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
