

Association of Serum Soluble Urokinase Receptor Levels With Progression of Kidney Disease in Children
- PMID: 28873129
- PMCID: PMC6121753
- DOI: 10.1001/jamapediatrics.2017.2914
Association of Serum Soluble Urokinase Receptor Levels With Progression of Kidney Disease in Children
Erratum in
-
Error in Table Data.JAMA Pediatr. 2017 Nov 1;171(11):1127. doi: 10.1001/jamapediatrics.2017.3864. JAMA Pediatr. 2017. PMID: 29052685 Free PMC article. No abstract available.
Abstract
Importance: Conventional methods to diagnose and monitor chronic kidney disease (CKD) in children, such as creatinine level and cystatin C-derived estimated glomerular filtration rate (eGFR) and assessment of proteinuria in spot or timed urine samples, are of limited value in identifying patients at risk of progressive kidney function loss. Serum soluble urokinase receptor (suPAR) levels strongly predict incident CKD stage 3 in adults.
Objective: To determine whether elevated suPAR levels are associated with renal disease progression in children with CKD.
Design, setting, and participants: Post hoc analysis of 2 prospectively followed up pediatric CKD cohorts, ie, the ESCAPE Trial (1999-2007) and the 4C Study (2010-2016), with serum suPAR level measured at enrollment and longitudinal eGFR measured prospectively. In the 2 trials, a total of 898 children were observed at 30 (ESCAPE Trial; n = 256) and 55 (4C Study; n = 642) tertiary care hospitals in 13 European countries. Renal diagnoses included congenital anomalies of the kidneys and urinary tract (n = 637 [70.9%]), tubulointerstitial nephropathies (n = 92 [10.2%]), glomerulopathies (n = 69 [7.7%]), postischemic CKD (n = 42 [4.7%]), and other CKD (n = 58 [6.5%]). Total follow-up duration was up to 7.9 years, and median follow-up was 3.1 years. Analyses were conducted from October 2016 to December 2016.
Exposures: Serum suPAR level was measured at enrollment, and eGFR was measured every 2 months in the ESCAPE Trial and every 6 months in the 4C Study. The primary end point of CKD progression was a composite of 50% eGFR loss, eGFR less than 10 mL/min/1.73 m2, or initiation of renal replacement therapy.
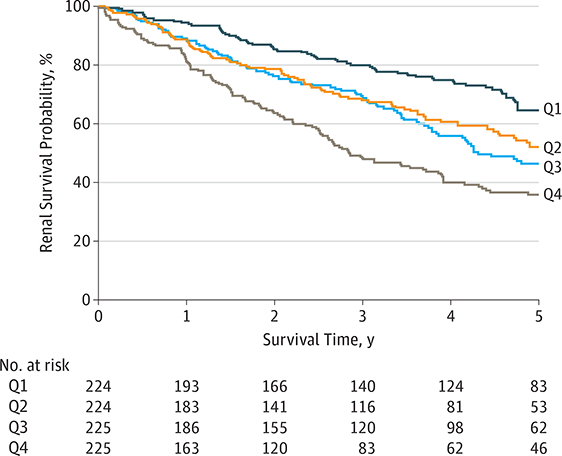
Main outcomes and measures: The primary end point in this study was renal survival, defined as a composite of 50% loss of GFR that persisted for at least 1 month, the start of renal replacement therapy, or an eGFR less than 10 mL/min/1.73 m2.
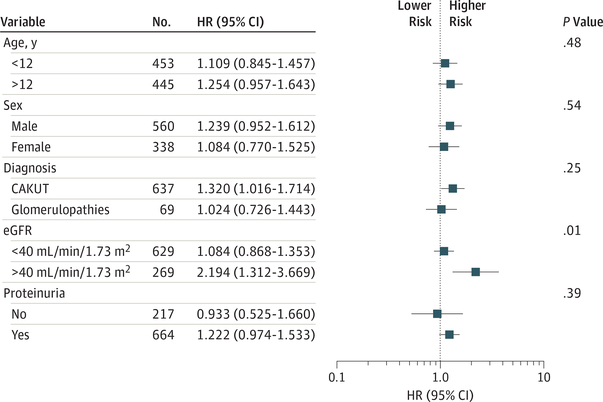
Results: Of the 898 included children, 560 (62.4%) were male, and the mean (SD) patient age at enrollment was 11.9 (3.5) years. The mean (SD) eGFR was 34 (16) mL/min/1.73 m2. The 5-year end point-free renal survival was 64.5% (95% CI, 57.4-71.7) in children with suPAR levels in the lowest quartile compared with 35.9% (95% CI, 28.7-43.0) in those in the highest quartile (P < .001). By multivariable analysis, the risk of attaining the end point was higher in children with glomerulopathies and increased with age, blood pressure, proteinuria, and lower eGFR at baseline. In patients with baseline eGFR greater than 40 mL/min/1.73 m2, higher log-transformed suPAR levels were associated with a higher risk of CKD progression after adjustment for traditional risk factors (hazard ratio, 5.12; 95% CI, 1.56-16.7; P = .007).
Conclusions and relevance: Patients with high suPAR levels were more likely to have progression of their kidney disease. Further studies should determine whether suPAR levels can identify children at risk for future CKD.
Figures
References
-
- Wühl E, Trivelli A, Picca S, et al. ; ESCAPE Trial Group. Strict blood-pressure control and progression of renal failure in children. N Engl J Med. 2009;361(17):1639–1650. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
