

Association of Evidence-Based Care Processes With Mortality in Staphylococcus aureus Bacteremia at Veterans Health Administration Hospitals, 2003-2014
- PMID: 28873140
- PMCID: PMC5710211
- DOI: 10.1001/jamainternmed.2017.3958
Association of Evidence-Based Care Processes With Mortality in Staphylococcus aureus Bacteremia at Veterans Health Administration Hospitals, 2003-2014
Erratum in
-
Extraneous Sentence in the Abstract.JAMA Intern Med. 2017 Oct 1;177(10):1544. doi: 10.1001/jamainternmed.2017.6121. JAMA Intern Med. 2017. PMID: 28973265 Free PMC article. No abstract available.
Abstract
Importance: Staphylococcus aureus bacteremia is common and frequently associated with poor outcomes. Evidence indicates that specific care processes are associated with improved outcomes for patients with S aureus bacteremia, including appropriate antibiotic prescribing, use of echocardiography to identify endocarditis, and consultation with infectious diseases (ID) specialists. Whether use of these care processes has increased in routine care for S aureus bacteremia or whether use of these processes has led to large-scale improvements in survival is unknown.
Objective: To examine the association of evidence-based care processes in routine care for S aureus bacteremia with mortality.
Design, setting, and participants: This retrospective observational cohort study examined all patients admitted to Veterans Health Administration (VHA) acute care hospitals who had a first episode of S aureus bacteremia from January 1, 2003, through December 31, 2014.
Exposures: Use of appropriate antibiotic therapy, echocardiography, and ID consultation.
Main outcomes and measures: Thirty-day all-cause mortality.
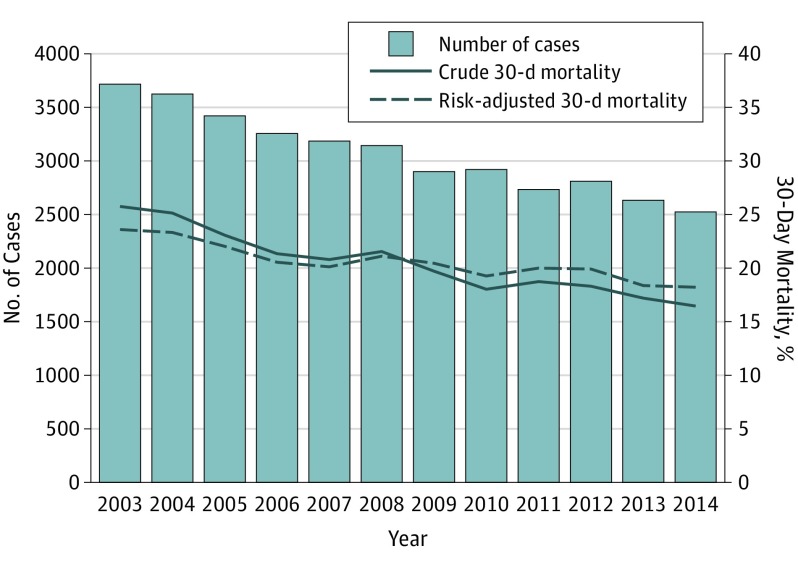
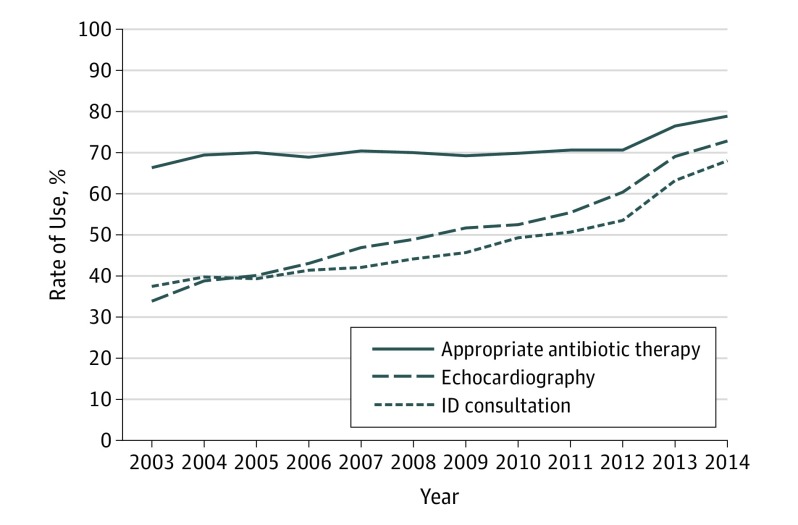
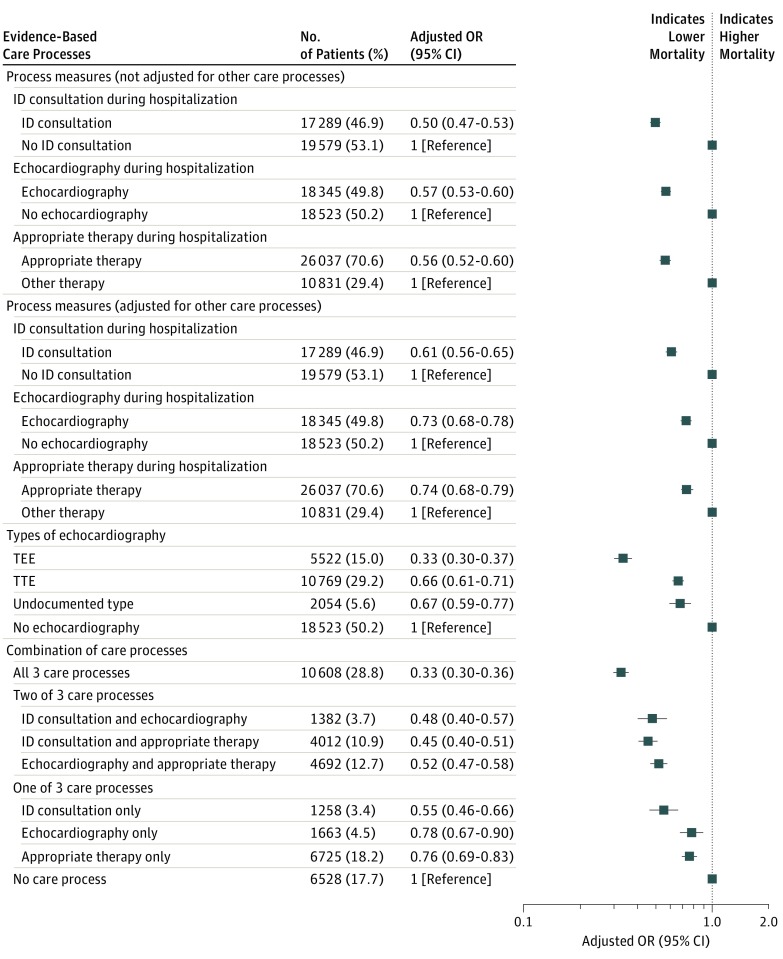
Results: Analyses included 36 868 patients in 124 hospitals (mean [SD] age, 66.4 [12.5] years; 36 036 [97.7%] male), including 19 325 (52.4%) with infection due to methicillin-resistant S aureus and 17 543 (47.6%) with infection due to methicillin-susceptible S aureus. Risk-adjusted mortality decreased from 23.5% (95% CI, 23.3%-23.8%) in 2003 to 18.2% (95% CI, 17.9%-18.5%) in 2014. Rates of appropriate antibiotic prescribing increased from 2467 (66.4%) to 1991 (78.9%), echocardiography from 1256 (33.8%) to 1837 (72.8%), and ID consultation from 1390 (37.4%) to 1717 (68.0%). After adjustment for patient characteristics, cohort year, and other care processes, receipt of care processes was associated with lower mortality, with adjusted odds ratios of 0.74 (95% CI, 0.68-0.79) for appropriate antibiotics, 0.73 (95% CI, 0.68-0.78) for echocardiography, and 0.61 (95% CI, 0.56-0.65) for ID consultation. Mortality decreased progressively as the number of care processes that a patient received increased (adjusted odds ratio for all 3 processes compared with none, 0.33; 95% CI, 0.30-0.36). An estimated 57.3% (95% CI, 48.4%-69.9%) of the decrease in mortality between 2003 and 2014 could be attributed to increased use of these evidence-based care processes.
Conclusions and relevance: Mortality associated with S aureus bacteremia decreased significantly in VHA hospitals, and a substantial portion of the decreasing mortality may have been attributable to increased use of evidence-based care processes. The experience in VHA hospitals demonstrates that increasing application of these care processes may improve survival among patients with S aureus bacteremia in routine health care settings.
Conflict of interest statement
Figures
Comment in
-
Immortal Time Bias in Assessing Evidence-Based Care Processes for Staphylococcus aureus Bacteremia.JAMA Intern Med. 2018 Feb 1;178(2):295-296. doi: 10.1001/jamainternmed.2017.7947. JAMA Intern Med. 2018. PMID: 29404611 No abstract available.
-
Immortal Time Bias in Assessing Evidence-Based Care Processes for Staphylococcus aureus Bacteremia-Reply.JAMA Intern Med. 2018 Feb 1;178(2):296. doi: 10.1001/jamainternmed.2017.7950. JAMA Intern Med. 2018. PMID: 29404616 No abstract available.
References
-
- Laupland KB, Lyytikäinen O, Søgaard M, et al. ; International Bacteremia Surveillance Collaborative . The changing epidemiology of Staphylococcus aureus bloodstream infection: a multinational population-based surveillance study. Clin Microbiol Infect. 2013;19(5):465-471. - PubMed
-
- Frimodt-Møller N, Espersen F, Skinhøj P, Rosdahl VT. Epidemiology of Staphylococcus aureus bacteremia in Denmark from 1957 to 1990. Clin Microbiol Infect. 1997;3(3):297-305. - PubMed
-
- Tom S, Galbraith JC, Valiquette L, et al. ; International Bacteraemia Surveillance Collaborative . Case fatality ratio and mortality rate trends of community-onset Staphylococcus aureus bacteraemia. Clin Microbiol Infect. 2014;20(10):O630-O632. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
