

Effect of Colonoscopy Outreach vs Fecal Immunochemical Test Outreach on Colorectal Cancer Screening Completion: A Randomized Clinical Trial
- PMID: 28873161
- PMCID: PMC5648645
- DOI: 10.1001/jama.2017.11389
Effect of Colonoscopy Outreach vs Fecal Immunochemical Test Outreach on Colorectal Cancer Screening Completion: A Randomized Clinical Trial
Abstract
Importance: Mailed fecal immunochemical test (FIT) outreach is more effective than colonoscopy outreach for increasing 1-time colorectal cancer (CRC) screening, but long-term effectiveness may need repeat testing and timely follow-up for abnormal results.
Objective: Compare the effectiveness of FIT outreach and colonoscopy outreach to increase completion of the CRC screening process (screening initiation and follow-up) within 3 years.
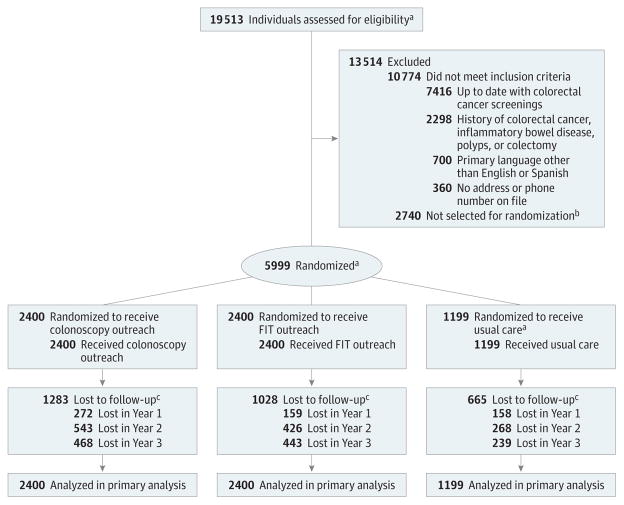
Design, setting, and participants: Pragmatic randomized clinical trial from March 2013 to July 2016 among 5999 participants aged 50 to 64 years who were receiving primary care in Parkland Health and Hospital System and were not up to date with CRC screenings.
Interventions: Random assignment to mailed FIT outreach (n = 2400), mailed colonoscopy outreach (n = 2400), or usual care with clinic-based screening (n = 1199). Outreach included processes to promote repeat annual testing for individuals in the FIT outreach group with normal results and completion of diagnostic and screening colonoscopy for those with an abnormal FIT result or assigned to colonoscopy outreach.
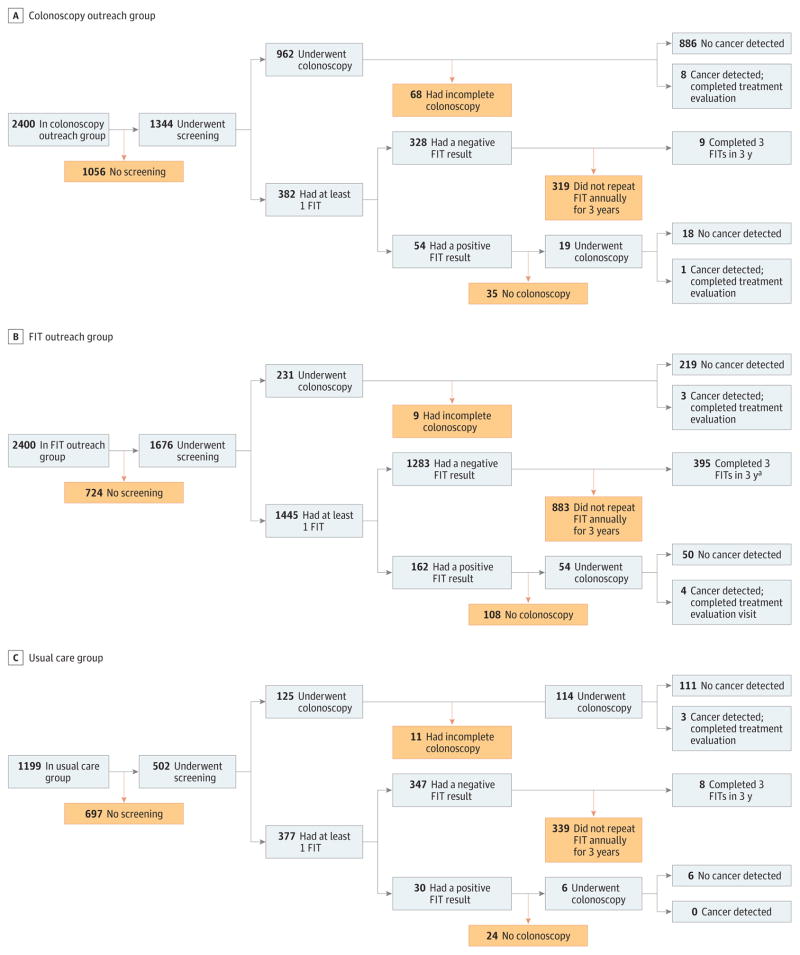
Main outcomes and measures: Primary outcome was screening process completion, defined as adherence to colonoscopy completion, annual testing for a normal FIT result, diagnostic colonoscopy for an abnormal FIT result, or treatment evaluation if CRC was detected. Secondary outcomes included detection of any adenoma or advanced neoplasia (including CRC) and screening-related harms (including bleeding or perforation).
Results: All 5999 participants (median age, 56 years; women, 61.9%) were included in the intention-to-screen analyses. Screening process completion was 38.4% in the colonoscopy outreach group, 28.0% in the FIT outreach group, and 10.7% in the usual care group. Compared with the usual care group, between-group differences for completion were higher for both outreach groups (27.7% [95% CI, 25.1% to 30.4%] for the colonoscopy outreach group; 17.3% [95% CI, 14.8% to 19.8%] for FIT outreach group), and highest in the colonoscopy outreach group (10.4% [95% CI, 7.8% to 13.1%] for the colonoscopy outreach group vs FIT outreach group; P < .001 for all comparisons). Compared with usual care, the between-group differences in adenoma and advanced neoplasia detection rates were higher for both outreach groups (colonoscopy outreach group: 10.3% [95% CI, 9.5% to 12.1%] for adenoma and 3.1% [95% CI, 2.0% to 4.1%] for advanced neoplasia, P < .001 for both comparisons; FIT outreach group: 1.3% [95% CI, -0.1% to 2.8%] for adenoma and 0.7% [95% CI, -0.2% to 1.6%] for advanced neoplasia, P < .08 and P < .13, respectively), and highest in the colonoscopy outreach group (colonoscopy outreach group vs FIT outreach group: 9.0% [95% CI, 7.3% to 10.7%] for adenoma and 2.4% [95% CI, 1.3% to 3.3%] for advanced neoplasia, P < .001 for both comparisons). There were no screening-related harms in any groups.
Conclusions and relevance: Among persons aged 50 to 64 years receiving primary care at a safety-net institution, mailed outreach invitations offering FIT or colonoscopy compared with usual care increased the proportion completing CRC screening process within 3 years. The rate of screening process completion was higher with colonoscopy than FIT outreach.
Trial registration: clinicaltrials.gov Identifier: NCT01710215.
Conflict of interest statement
Figures
Comment in
-
Using Outreach to Improve Colorectal Cancer Screening.JAMA. 2017 Sep 5;318(9):799-800. doi: 10.1001/jama.2017.10606. JAMA. 2017. PMID: 28873142 No abstract available.
-
Colonoscopy outreach increased CRC screening more than FIT outreach; both were better than usual care.Ann Intern Med. 2017 Dec 19;167(12):JC65. doi: 10.7326/ACPJC-2017-167-12-065. Ann Intern Med. 2017. PMID: 29255855 No abstract available.
References
-
- Bibbins-Domingo K, Grossman DC, Curry SJ, et al. US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2016;315(23):2564–2575. - PubMed
-
- Liss DT, Petit-Homme A, Feinglass J, Buchanan DR, Baker DW. Adherence to repeat fecal occult blood testing in an urban community health center network. J Community Health. 2013;38(5):829–833. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
