

Mutation Detection in Patients With Advanced Cancer by Universal Sequencing of Cancer-Related Genes in Tumor and Normal DNA vs Guideline-Based Germline Testing
- PMID: 28873162
- PMCID: PMC5611881
- DOI: 10.1001/jama.2017.11137
Mutation Detection in Patients With Advanced Cancer by Universal Sequencing of Cancer-Related Genes in Tumor and Normal DNA vs Guideline-Based Germline Testing
Erratum in
-
Missing Conflict of Interest Disclosure.JAMA. 2018 Dec 11;320(22):2381. doi: 10.1001/jama.2018.17511. JAMA. 2018. PMID: 30422164 Free PMC article. No abstract available.
Abstract
Importance: Guidelines for cancer genetic testing based on family history may miss clinically actionable genetic changes with established implications for cancer screening or prevention.
Objective: To determine the proportion and potential clinical implications of inherited variants detected using simultaneous sequencing of the tumor and normal tissue ("tumor-normal sequencing") compared with genetic test results based on current guidelines.
Design, setting, and participants: From January 2014 until May 2016 at Memorial Sloan Kettering Cancer Center, 10 336 patients consented to tumor DNA sequencing. Since May 2015, 1040 of these patients with advanced cancer were referred by their oncologists for germline analysis of 76 cancer predisposition genes. Patients with clinically actionable inherited mutations whose genetic test results would not have been predicted by published decision rules were identified. Follow-up for potential clinical implications of mutation detection was through May 2017.
Exposure: Tumor and germline sequencing compared with the predicted yield of targeted germline sequencing based on clinical guidelines.
Main outcomes and measures: Proportion of clinically actionable germline mutations detected by universal tumor-normal sequencing that would not have been detected by guideline-directed testing.
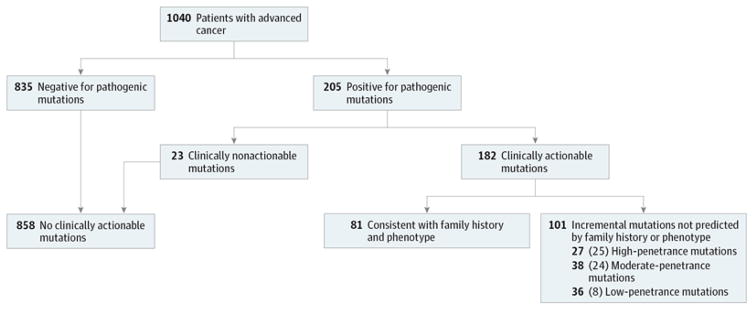
Results: Of 1040 patients, the median age was 58 years (interquartile range, 50.5-66 years), 65.3% were male, and 81.3% had stage IV disease at the time of genomic analysis, with prostate, renal, pancreatic, breast, and colon cancer as the most common diagnoses. Of the 1040 patients, 182 (17.5%; 95% CI, 15.3%-19.9%) had clinically actionable mutations conferring cancer susceptibility, including 149 with moderate- to high-penetrance mutations; 101 patients tested (9.7%; 95% CI, 8.1%-11.7%) would not have had these mutations detected using clinical guidelines, including 65 with moderate- to high-penetrance mutations. Frequency of inherited mutations was related to case mix, stage, and founder mutations. Germline findings led to discussion or initiation of change to targeted therapy in 38 patients tested (3.7%) and predictive testing in the families of 13 individuals (1.3%), including 6 for whom genetic evaluation would not have been initiated by guideline-based testing.
Conclusions and relevance: In this referral population with selected advanced cancers, universal sequencing of a broad panel of cancer-related genes in paired germline and tumor DNA samples was associated with increased detection of individuals with potentially clinically significant heritable mutations over the predicted yield of targeted germline testing based on current clinical guidelines. Knowledge of these additional mutations can help guide therapeutic and preventive interventions, but whether all of these interventions would improve outcomes for patients with cancer or their family members requires further study.
Trial registration: clinicaltrials.gov Identifier: NCT01775072.
Conflict of interest statement
Figures
Comment in
-
The Potential and Challenges of Expanded Germline Testing in Clinical Oncology.JAMA. 2017 Sep 5;318(9):801-803. doi: 10.1001/jama.2017.11022. JAMA. 2017. PMID: 28873143 No abstract available.
-
Failure to Disclose Conflict of Interest in Article Published in JAMA on Detection of Cancer-Related Genes.JAMA. 2018 Dec 11;320(22):2380. doi: 10.1001/jama.2018.16961. JAMA. 2018. PMID: 30422165 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
