

Evaluating a Dutch cardiology primary care plus intervention on the Triple Aim outcomes: study design of a practice-based quantitative and qualitative research
- PMID: 28874148
- PMCID: PMC5585935
- DOI: 10.1186/s12913-017-2580-x
Evaluating a Dutch cardiology primary care plus intervention on the Triple Aim outcomes: study design of a practice-based quantitative and qualitative research
Abstract
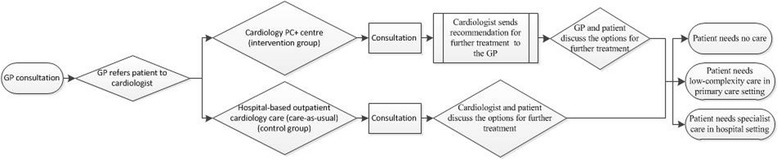
Background: In an attempt to deal with the pressures on the health-care system and to guarantee sustainability, changes are needed. This study focuses on a cardiology primary care plus intervention. Primary care plus (PC+) is a new health-care delivery model focused on substitution of specialist care in the hospital setting with specialist care in the primary care setting. The intervention consists of a cardiology PC+ centre in which cardiologists, supported by other health-care professionals, provide consultations in a primary care setting. The PC+ centre aims to improve the health of the population and quality of care as experienced by patients, and reduce the number of referrals to hospital-based outpatient specialist care in order to reduce health-care costs. These aims reflect the Triple Aim principle. Hence, the objectives of the study are to evaluate the cardiology PC+ centre in terms of the Triple Aim outcomes and to evaluate the process of the introduction of PC+.
Methods/design: The study is a practice-based, quantitative study with a longitudinal observational design, and an additional qualitative study to supplement, interpret and improve the quantitative study. The study population of the quantitative part will consist of adult patients (≥18 years) with non-acute and low-complexity cardiology-related health complaints, who will be referred to the cardiology PC+ centre (intervention group) or hospital-based outpatient cardiology care (control group). All eligible patients will be asked to complete questionnaires at three different time points consisting of questions about their demographics, health status and experience of care. Additionally, quantitative data will be collected about health-care utilization and related health-care costs at the PC+ centre and the hospital. The qualitative part, consisting of semi-structured interviews, focus groups, and observations, is designed to evaluate the process as well as to amplify, clarify and explain quantitative results.
Conclusions: This study will evaluate a cardiology PC+ centre using quantitative and supplementary qualitative methods. The findings of both sub-studies will fill a gap in knowledge about the effects of PC+ and in particular whether PC+ is able to pursue the Triple Aim outcomes.
Trial registration: NTR6629 (Data registered: 25-08-2017) (registered retrospectively).
Keywords: Cardiology; Hospital care; Primary care; Primary care plus; Referral; Substitution; Triple Aim.
Conflict of interest statement
Ethics approval and consent to participate
The study is approved by the Medical Research and Ethics Committee of the Maastricht University Medical Centre, Maastricht, the Netherlands in 2015 (METC 15–4-032). Informed consent will be obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Porter ME, Teisberg EO. Redefining health care: creating value-based competition on results. United States: Harvard Business Press; 2006.
-
- Sociaal-Economische Raad (SER) Naar een kwalitatief goede, toegankelijke en betaalbare zorg: Een tussenadvies op hoofdlijnen. Den Haag: SER; 2012.
-
- van Ewijk C, van der Horst A, Besseling P. Toekomst voor de zorg. Den Haag: CPB; 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
