

Radiation-free CMR diagnostic heart catheterization in children
- PMID: 28874164
- PMCID: PMC5585983
- DOI: 10.1186/s12968-017-0374-2
Radiation-free CMR diagnostic heart catheterization in children
Abstract
Background: Children with heart disease may require repeated X-Ray cardiac catheterization procedures, are more radiosensitive, and more likely to survive to experience oncologic risks of medical radiation. Cardiovascular magnetic resonance (CMR) is radiation-free and offers information about structure, function, and perfusion but not hemodynamics. We intend to perform complete radiation-free diagnostic right heart catheterization entirely using CMR fluoroscopy guidance in an unselected cohort of pediatric patients; we report the feasibility and safety.
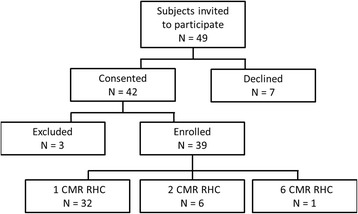
Methods: We performed 50 CMR fluoroscopy guided comprehensive transfemoral right heart catheterizations in 39 pediatric (12.7 ± 4.7 years) subjects referred for clinically indicated cardiac catheterization. CMR guided catheterizations were assessed by completion (success/failure), procedure time, and safety events (catheterization, anesthesia). Pre and post CMR body temperature was recorded. Concurrent invasive hemodynamic and diagnostic CMR data were collected.
Results: During a twenty-two month period (3/2015 - 12/2016), enrolled subjects had the following clinical indications: post-heart transplant 33%, shunt 28%, pulmonary hypertension 18%, cardiomyopathy 15%, valvular heart disease 3%, and other 3%. Radiation-free CMR guided right heart catheterization attempts were all successful using passive catheters. In two subjects with septal defects, right and left heart catheterization were performed. There were no complications. One subject had six such procedures. Most subjects (51%) had undergone multiple (5.5 ± 5) previous X-Ray cardiac catheterizations. Retained thoracic surgical or transcatheter implants (36%) did not preclude successful CMR fluoroscopy heart catheterization. During the procedure, two subjects were receiving vasopressor infusions at baseline because of poor cardiac function, and in ten procedures, multiple hemodynamic conditions were tested.
Conclusions: Comprehensive CMR fluoroscopy guided right heart catheterization was feasible and safe in this small cohort of pediatric subjects. This includes subjects with previous metallic implants, those requiring continuous vasopressor medication infusions, and those requiring pharmacologic provocation. Children requiring multiple, serial X-Ray cardiac catheterizations may benefit most from radiation sparing. This is a step toward wholly CMR guided diagnostic (right and left heart) cardiac catheterization and future CMR guided cardiac intervention.
Trial registration: ClinicalTrials.gov NCT02739087 registered February 17, 2016.
Keywords: Catheterization; Interventional Cardiovascular MRI; MRI fluoroscopy; Magnetic Resonance Imaging; Real-time MRI.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
The study was approved by the Children’s National Medical Center Institutional Review Board (CNMC IRB 3860). Parental consent (subject assent when appropriate) was obtained for all subjects in writing.
Consent for publication
The protocol includes permission to use de-identified subject images in scientific communications.
Competing interests
NIH and CNMC have collaborative research and development agreements for interventional cardiovascular MRI with Siemens Medical Systems.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
