

Variation in monitoring and treatment policies for intracranial hypertension in traumatic brain injury: a survey in 66 neurotrauma centers participating in the CENTER-TBI study
- PMID: 28874206
- PMCID: PMC5586023
- DOI: 10.1186/s13054-017-1816-9
Variation in monitoring and treatment policies for intracranial hypertension in traumatic brain injury: a survey in 66 neurotrauma centers participating in the CENTER-TBI study
Abstract
Background: No definitive evidence exists on how intracranial hypertension should be treated in patients with traumatic brain injury (TBI). It is therefore likely that centers and practitioners individually balance potential benefits and risks of different intracranial pressure (ICP) management strategies, resulting in practice variation. The aim of this study was to examine variation in monitoring and treatment policies for intracranial hypertension in patients with TBI.
Methods: A 29-item survey on ICP monitoring and treatment was developed on the basis of literature and expert opinion, and it was pilot-tested in 16 centers. The questionnaire was sent to 68 neurotrauma centers participating in the Collaborative European Neurotrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) study.
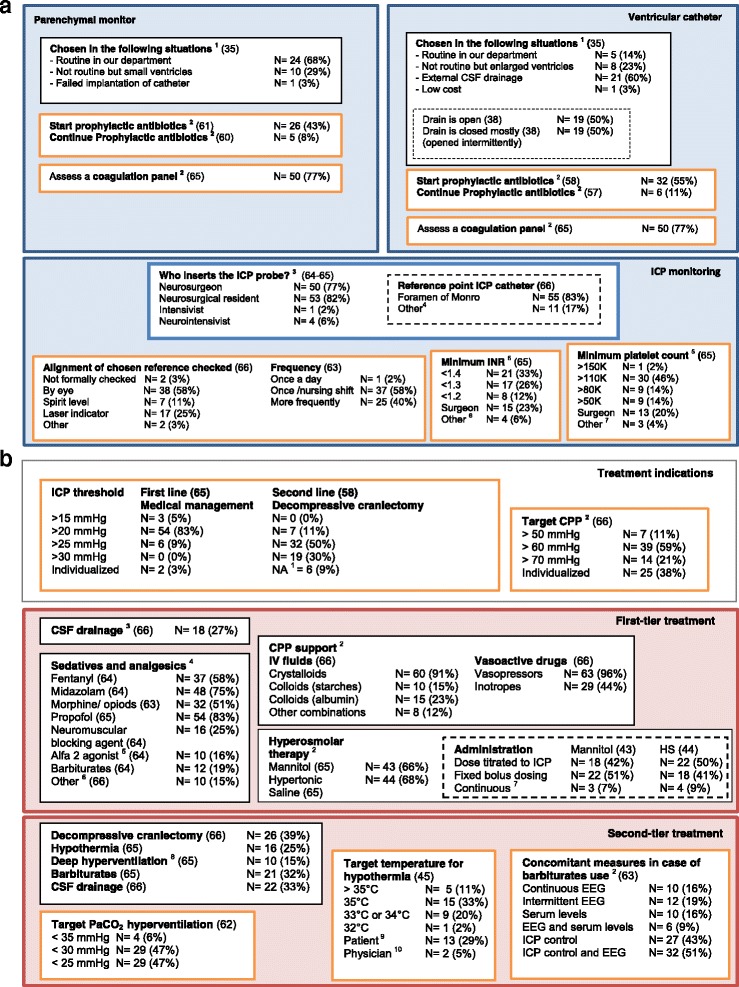
Results: The survey was completed by 66 centers (97% response rate). Centers were mainly academic hospitals (n = 60, 91%) and designated level I trauma centers (n = 44, 67%). The Brain Trauma Foundation guidelines were used in 49 (74%) centers. Approximately 90% of the participants (n = 58) indicated placing an ICP monitor in patients with severe TBI and computed tomographic abnormalities. There was no consensus on other indications or on peri-insertion precautions. We found wide variation in the use of first- and second-tier treatments for elevated ICP. Approximately half of the centers were classified as using a relatively aggressive approach to ICP monitoring and treatment (n = 32, 48%), whereas the others were considered more conservative (n = 34, 52%).
Conclusions: Substantial variation was found regarding monitoring and treatment policies in patients with TBI and intracranial hypertension. The results of this survey indicate a lack of consensus between European neurotrauma centers and provide an opportunity and necessity for comparative effectiveness research.
Keywords: Comparative effectiveness research; ICP; ICU; Intracranial hypertension; Survey; Traumatic brain injury.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable. There are no patients included in present study, and participating centers have given consent by completing the questionnaires.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Comment in
-
Breaking the rules: is it the neurointensivists' turn?Crit Care. 2018 Jan 29;22(1):21. doi: 10.1186/s13054-017-1919-3. Crit Care. 2018. PMID: 29378635 Free PMC article. No abstract available.
References
-
- Bosco JL, Silliman RA, Thwin SS, Geiger AM, Buist DS, Prout MN, Yood MU, Haque R, Wei F, Lash TL. A most stubborn bias: no adjustment method fully resolves confounding by indication in observational studies. J Clin Epidemiol. 2010;63(1):64–74. doi: 10.1016/j.jclinepi.2009.03.001. - DOI - PMC - PubMed
