

A Phase II Trial of Neoadjuvant MK-2206, an AKT Inhibitor, with Anastrozole in Clinical Stage II or III PIK3CA-Mutant ER-Positive and HER2-Negative Breast Cancer
- PMID: 28874413
- PMCID: PMC6392430
- DOI: 10.1158/1078-0432.CCR-17-1260
A Phase II Trial of Neoadjuvant MK-2206, an AKT Inhibitor, with Anastrozole in Clinical Stage II or III PIK3CA-Mutant ER-Positive and HER2-Negative Breast Cancer
Abstract
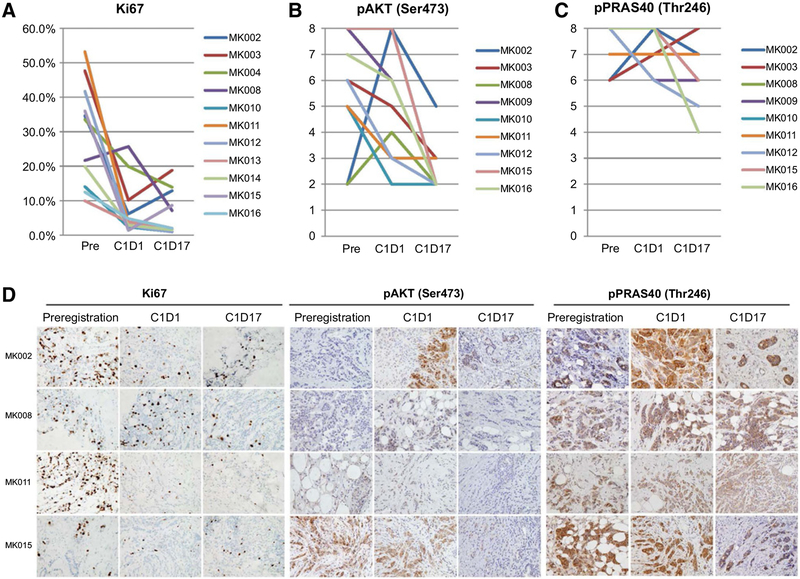
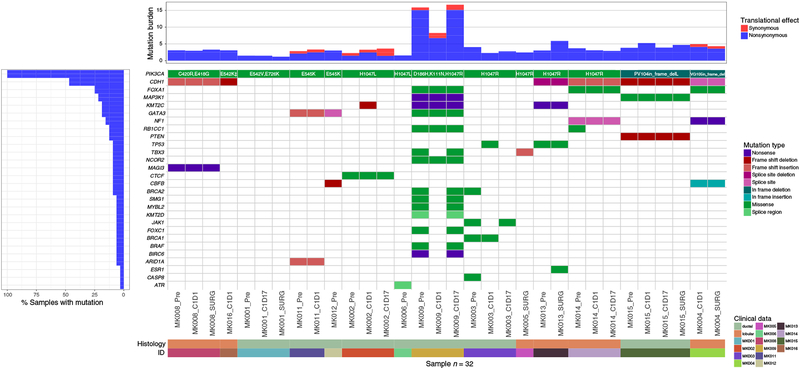
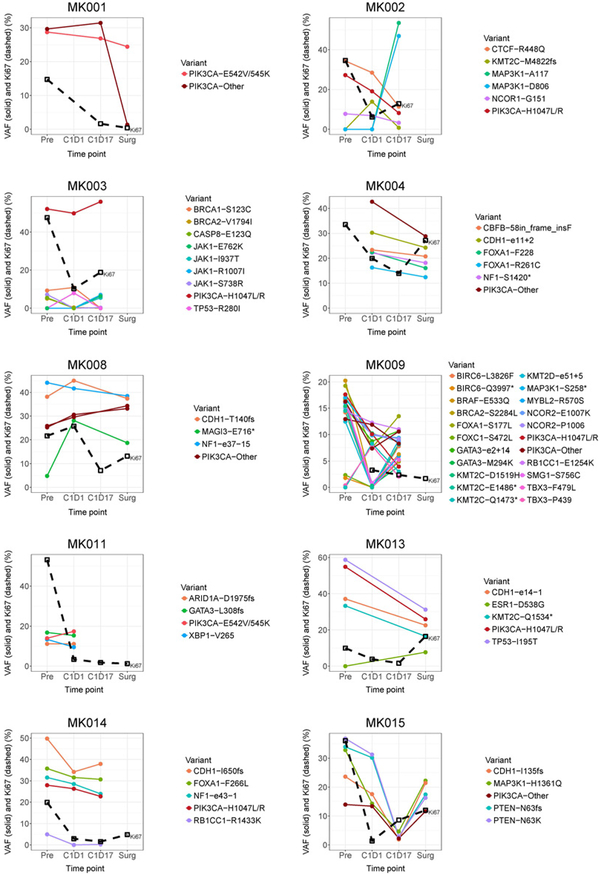
Purpose: Hyperactivation of AKT is common and associated with endocrine resistance in estrogen receptor-positive (ER+) breast cancer. The allosteric pan-AKT inhibitor MK-2206 induced apoptosis in PIK3CA-mutant ER+ breast cancer under estrogen-deprived condition in preclinical studies. This neoadjuvant phase II trial was therefore conducted to test the hypothesis that adding MK-2206 to anastrozole induces pathologic complete response (pCR) in PIK3CA mutant ER+ breast cancer.Experimental Design: Potential eligible patients with clinical stage II/III ER+/HER2- breast cancer were preregistered and received anastrozole (goserelin if premenopausal) for 28 days in cycle 0 pending tumor PIK3CA sequencing. Patients positive for PIK3CA mutation in the tumor were eligible to start MK-2206 (150 mg orally weekly, with prophylactic prednisone) on cycle 1 day 2 (C1D2) and to receive a maximum of four 28-day cycles of combination therapy before surgery. Serial biopsies were collected at preregistration, C1D1 and C1D17.Results: Fifty-one patients preregistered and 16 of 22 with PIK3CA-mutant tumors received study drug. Three patients went off study due to C1D17 Ki67 >10% (n = 2) and toxicity (n = 1). Thirteen patients completed neoadjuvant therapy followed by surgery. No pCRs were observed. Rash was common. MK-2206 did not further suppress cell proliferation and did not induce apoptosis on C1D17 biopsies. Although AKT phosphorylation was reduced, PRAS40 phosphorylation at C1D17 after MK-2206 persisted. One patient acquired an ESR1 mutation at surgery.Conclusions: MK-2206 is unlikely to add to the efficacy of anastrozole alone in PIK3CA-mutant ER+ breast cancer and should not be studied further in the target patient population. Clin Cancer Res; 23(22); 6823-32. ©2017 AACR.
©2017 American Association for Cancer Research.
Figures
References
-
- Houssami N, Macaskill P, von Minckwitz G, Marinovich ML, Mamounas E. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoadjuvant chemotherapy. Eur J Cancer 2012; 48:3342–54. - PubMed
-
- Dowsett M, Smith IE, Ebbs SR, Dixon JM, Skene A, Griffith C, et al. Proliferation and apoptosis as markers of benefit in neoadjuvant endocrine therapy of breast cancer. Clin Cancer Res 2006;12:1024s–30s. - PubMed
-
- Bonnefoi H, Litière S, Piccart M, MacGrogan G, Fumoleau P, Brain E, et al. Pathological complete response after neoadjuvant chemotherapy is an independent predictive factor irrespective of simplified breast cancer intrinsic subtypes: a landmark and two-step approach analyses from the EORTC 10994/BIG 1–00 phase III trial. Ann Oncol 2014;25:1128–36. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
