

Type 1 diabetes induction in humanized mice
- PMID: 28874533
- PMCID: PMC5642714
- DOI: 10.1073/pnas.1710415114
Type 1 diabetes induction in humanized mice
Abstract
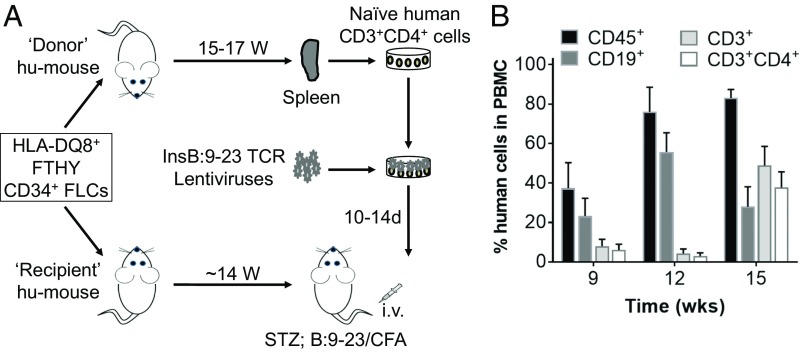
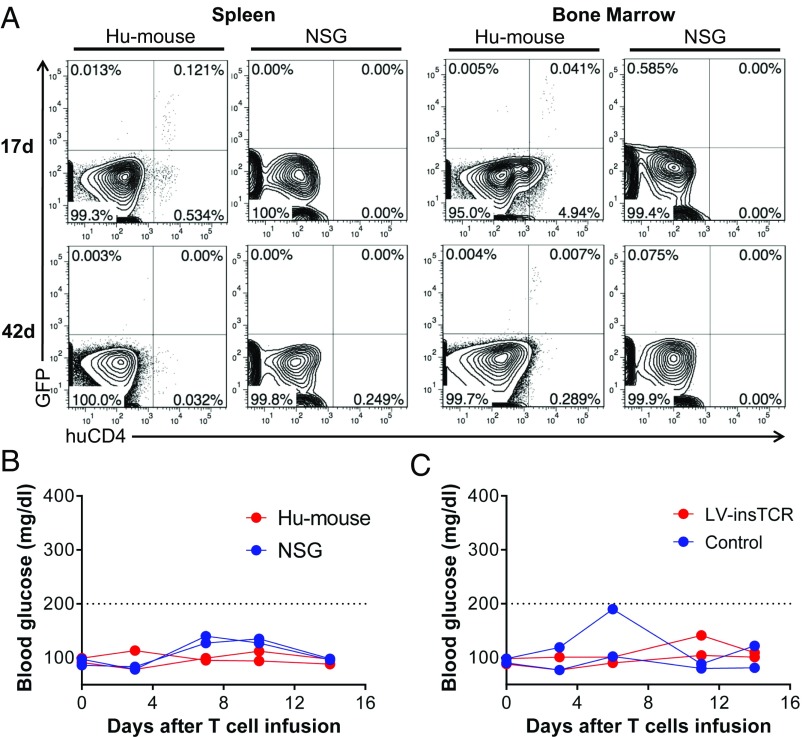
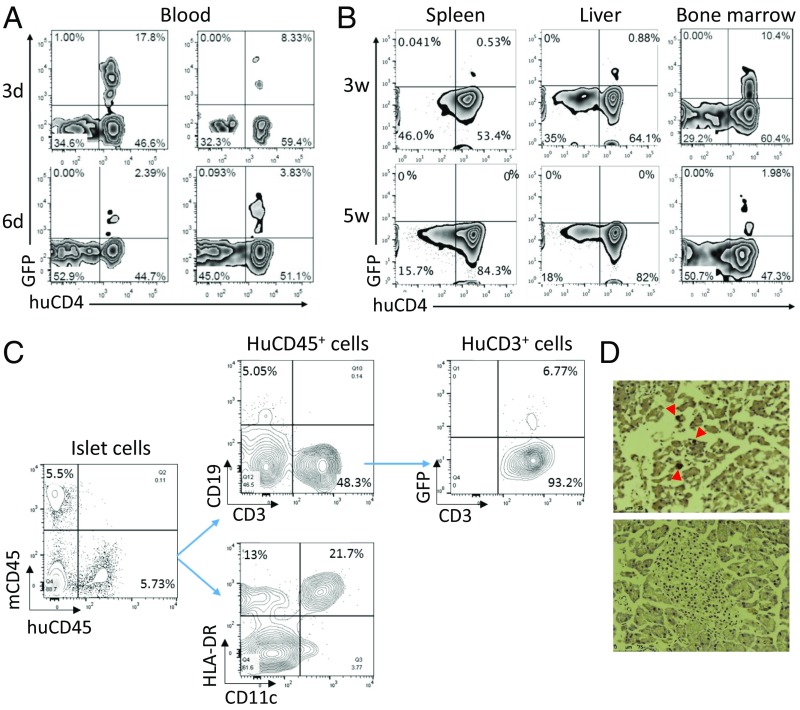
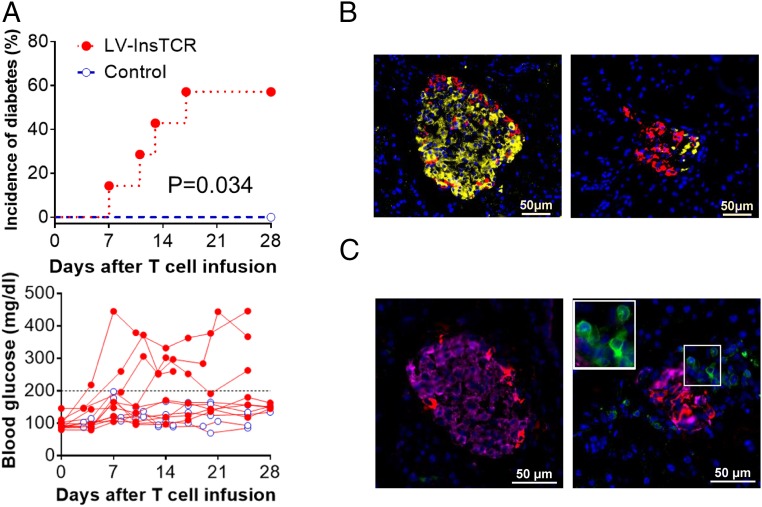
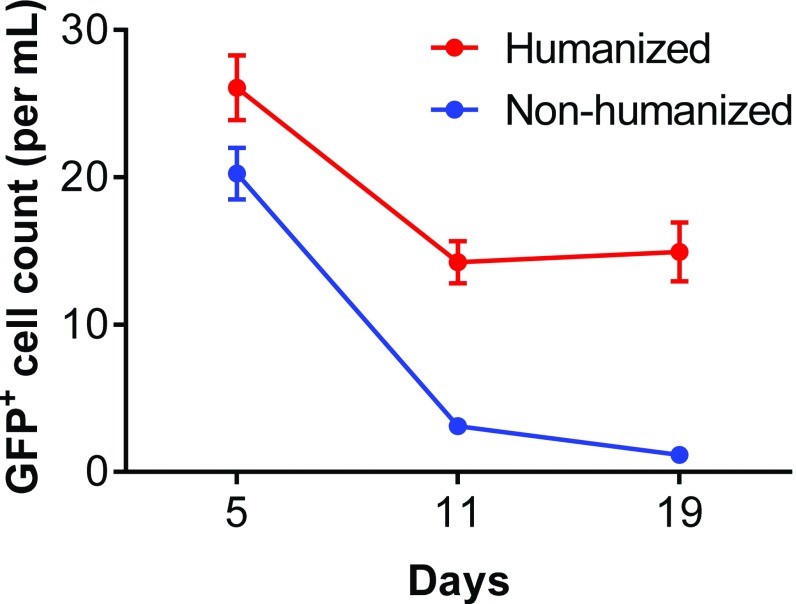
There is an urgent and unmet need for humanized in vivo models of type 1 diabetes to study immunopathogenesis and immunotherapy, and in particular antigen-specific therapy. Transfer of patient blood lymphocytes to immunodeficient mice is associated with xenogeneic graft-versus-host reactivity that complicates assessment of autoimmunity. Improved models could identify which human T cells initiate and participate in beta-cell destruction and help define critical target islet autoantigens. We used humanized mice (hu-mice) containing robust human immune repertoires lacking xenogeneic graft-versus-host reactivity to address this question. Hu-mice constructed by transplantation of HLA-DQ8+ human fetal thymus and CD34+ cells into HLA-DQ8-transgenic immunodeficient mice developed hyperglycemia and diabetes after transfer of autologous HLA-DQ8/insulin-B:9-23 (InsB:9-23)-specific T-cell receptor (TCR)-expressing human CD4+ T cells and immunization with InsB:9-23. Survival of the infused human T cells depended on the preexisting autologous human immune system, and pancreatic infiltration by human CD3+ T cells and insulitis were observed in the diabetic hu-mice, provided their islets were stressed by streptozotocin. This study fits Koch's postulate for pathogenicity, demonstrating a pathogenic role of islet autoreactive CD4+ T-cell responses in type 1 diabetes induction in humans, underscores the role of the target beta-cells in their immunological fate, and demonstrates the capacity to initiate disease with T cells, recognizing the InsB:9-23 epitope in the presence of islet inflammation. This preclinical model has the potential to be used in studies of the pathogenesis of type 1 diabetes and for testing of clinically relevant therapeutic interventions.
Keywords: humanized mice; insulin; type 1 diabetes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Comment in
-
Bridge between type 1 diabetes in mouse and man.Proc Natl Acad Sci U S A. 2017 Oct 10;114(41):10821-10823. doi: 10.1073/pnas.1715058114. Epub 2017 Oct 2. Proc Natl Acad Sci U S A. 2017. PMID: 28973949 Free PMC article. No abstract available.
References
-
- Roep BO, Atkinson M, von Herrath M. Satisfaction (not) guaranteed: Re-evaluating the use of animal models of type 1 diabetes. Nat Rev Immunol. 2004;4:989–997. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
