

Pediatric Patients Discharged from the Emergency Department with Abnormal Vital Signs
- PMID: 28874940
- PMCID: PMC5576624
- DOI: 10.5811/westjem.2017.5.33000
Pediatric Patients Discharged from the Emergency Department with Abnormal Vital Signs
Abstract
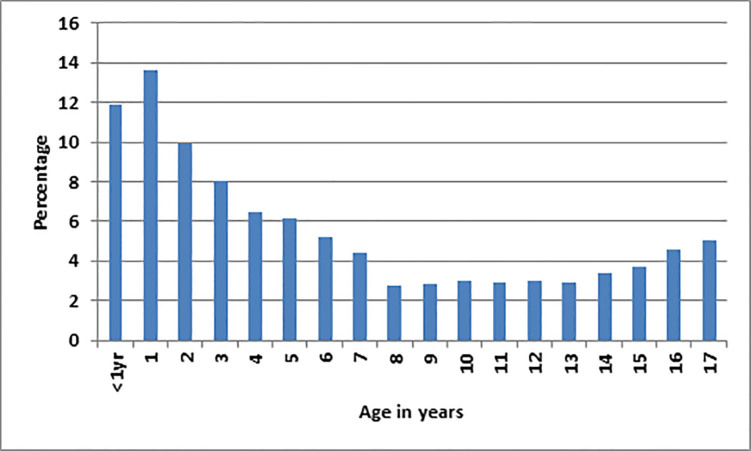
Introduction: Children often present to the emergency department (ED) with minor conditions such as fever and have persistently abnormal vital signs. We hypothesized that a significant portion of children discharged from the ED would have abnormal vital signs and that those discharged with abnormal vital signs would experience very few adverse events.
Methods: We performed a retrospective chart review encompassing a 44-month period of all pediatric patients (aged two months to 17 years) who were discharged from the ED with an abnormal pulse rate, respiratory rate, temperature, or oxygen saturation. We used a local quality assurance database to identify pre-defined adverse events after discharge in this population. Our primary aim was to determine the proportion of children discharged with abnormal vital signs and the frequency and nature of adverse events. Additionally, we performed a sub-analysis comparing the rate of adverse events in children discharged with normal vs. abnormal vital signs, as well as a standardized review of the nature of each adverse event.
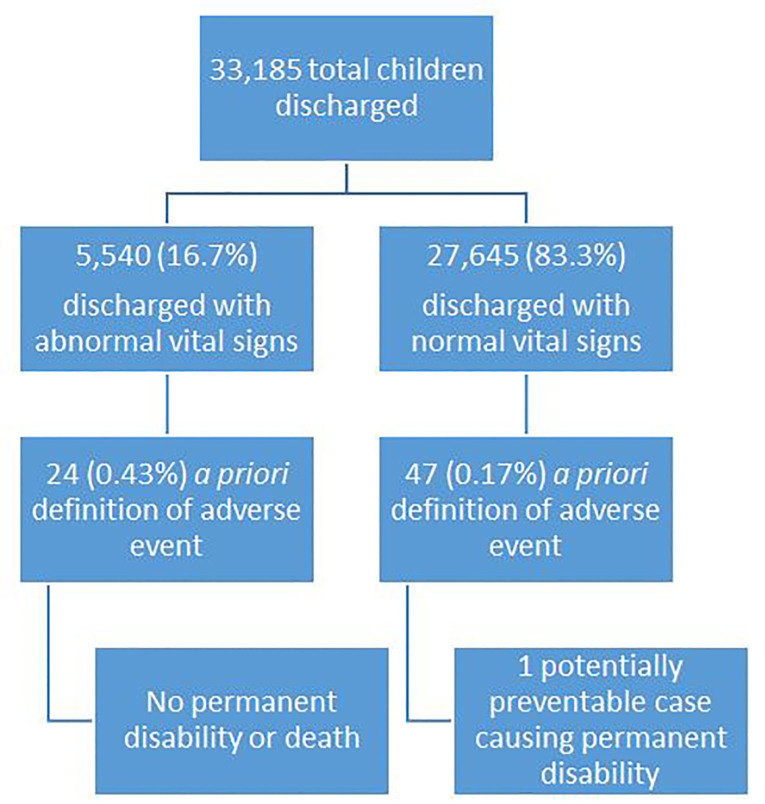
Results: Of 33,185 children discharged during the study period, 5,540 (17%) of these patients had at least one abnormal vital sign. There were 24/5,540 (0.43%) adverse events in the children with at least one abnormal vital sign vs. 47/27,645 (0.17%) adverse events in the children with normal vital signs [relative risk = 2.5 (95% confidence interval, 1.6 to 2.4)].However, upon review of each adverse event we found only one case that was related to the index visit, was potentially preventable by a 23-hour hospital observation, and caused permanent disability.
Conclusion: In our study population, 17% of the children were discharged with at least one abnormal vital sign, and there were very few adverse (0.43%) events associated with this practice. Heart rate was the most common abnormal vital sign leading to an adverse event. Severe adverse events that were potentially related to the abnormal vital sign(s) were exceedingly rare. Additional research is needed in broader populations to better determine the rate of adverse events and possible methods of avoiding them.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
References
-
- Hanna CM, Greenes DS. How much tachycardia in infants can be attributed to fever? Ann Emerg Med. 2004;43(6):699–705. - PubMed
-
- National Institute for Health and Care Excellence. Feverish illness in children—Assessment and initial management in children younger than 5 years. 2013. [Accessed October 17, 2015]. Available at: http://guidance.nice.org.uk/CG160/NICEGuidance/pdf/English.
-
- Thompson M, Coad N, Harnden A, et al. How well do vital signs identify children with serious infections in paediatric emergency care? Arch Dis Child. 2009;94(11):888–93. - PubMed
-
- Nijman RG, Zwinkels RL, van Veen M, et al. Can urgency classification of the manchester triage system predict serious bacterial infections in febrile children? Arch Dis Child. 2011;96(8):715–22. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical