

Duration of Mechanical Ventilation in the Emergency Department
- PMID: 28874952
- PMCID: PMC5576636
- DOI: 10.5811/westjem.2017.5.34099
Duration of Mechanical Ventilation in the Emergency Department
Abstract
Introduction: Due to hospital crowding, mechanically ventilated patients are increasingly spending hours boarding in emergency departments (ED) before intensive care unit (ICU) admission. This study aims to evaluate the association between time ventilated in the ED and in-hospital mortality, duration of mechanical ventilation, ICU and hospital length of stay (LOS).
Methods: This was a multi-center, prospective, observational study of patients ventilated in the ED, conducted at three academic Level I Trauma Centers from July 2011 to March 2013. All consecutive adult patients on invasive mechanical ventilation were eligible for enrollment. We performed a Cox regression to assess for a mortality effect for mechanically ventilated patients with each hour of increasing LOS in the ED and multivariable regression analyses to assess for independently significant contributors to in-hospital mortality. Our primary outcome was in-hospital mortality, with secondary outcomes of ventilator days, ICU LOS and hospital LOS. We further commented on use of lung protective ventilation and frequency of ventilator changes made in this cohort.
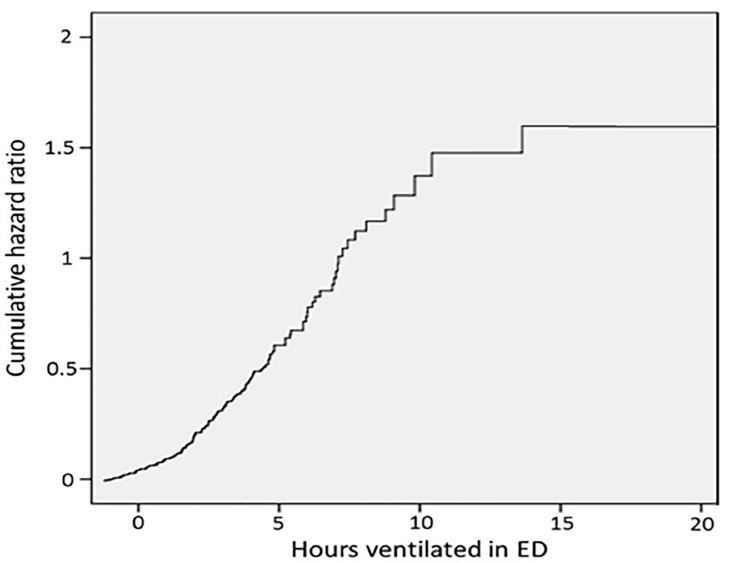
Results: We enrolled 535 patients, of whom 525 met all inclusion criteria. Altered mental status without respiratory pathology was the most common reason for intubation, followed by trauma and respiratory failure. Using iterated Cox regression, a mortality effect occurred at ED time of mechanical ventilation > 7 hours, and the longer ED stay was also associated with a longer total duration of intubation. However, adjusted multivariable regression analysis demonstrated only older age and admission to the neurosciences ICU as independently associated with increased mortality. Of interest, only 23.8% of patients ventilated in the ED for over seven hours had changes made to their ventilator.
Conclusion: In a prospective observational study of patients mechanically ventilated in the ED, there was a significant mortality benefit to expedited transfer of patients into an appropriate ICU setting.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. This study was funded in part by a university development grant. Dr. Sankoff is a section editor/decision editor/editorial board member of the Western Journal of Emergency Medicine. He had no role in the peer review process for this paper.
Figures
References
-
- Chalfin DB, Trzeciak S, Likourezos A, et al. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477–83. - PubMed
-
- Derlet RW, Richards JR. Overcrowding in the nation’s emergency departments: complex causes and disturbing effects. Ann Emerg Med. 2000;35(1):63–8. - PubMed
-
- Derlet RW, Richards JR. Emergency department overcrowding in Florida, New York, and Texas. South Med J. 2002;95(8):846–9. - PubMed
-
- Liew D, Liew D, Kennedy MP. Emergency department length of stay independently predicts excess inpatient length of stay. Med J Aust. 2003;179(10):524–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous