

Empirical Consequences of Current Recommendations for the Design and Interpretation of Noninferiority Trials
- PMID: 28875400
- PMCID: PMC5756156
- DOI: 10.1007/s11606-017-4161-4
Empirical Consequences of Current Recommendations for the Design and Interpretation of Noninferiority Trials
Abstract
Background: Noninferiority trials are increasingly common, though they have less standardized designs and their interpretation is less familiar to clinicians than superiority trials.
Objective: To empirically evaluate a cohort of noninferiority trials to determine 1) their interpretation as recommended by CONSORT, 2) choice of alpha threshold and its sidedness, and 3) differences between methods of analysis such as intention-to-treat and per-protocol.
Design: We searched MEDLINE for parallel-group randomized controlled noninferiority trials published in the five highest-impact general medical journals between 2011 and 2016.
Main measures: Data abstracted included trial design parameters, results, and interpretation of results based on CONSORT recommendations.
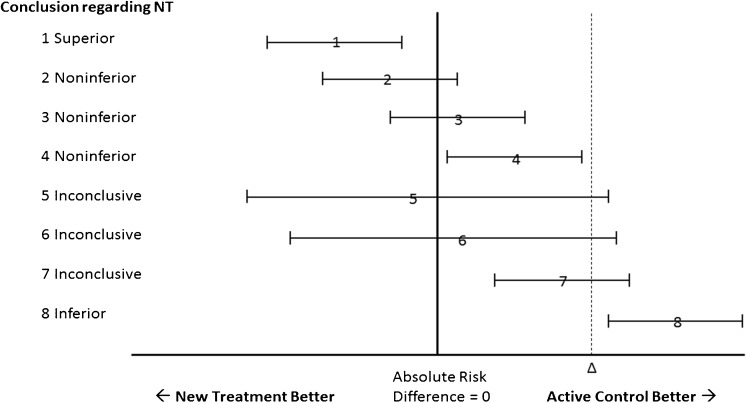
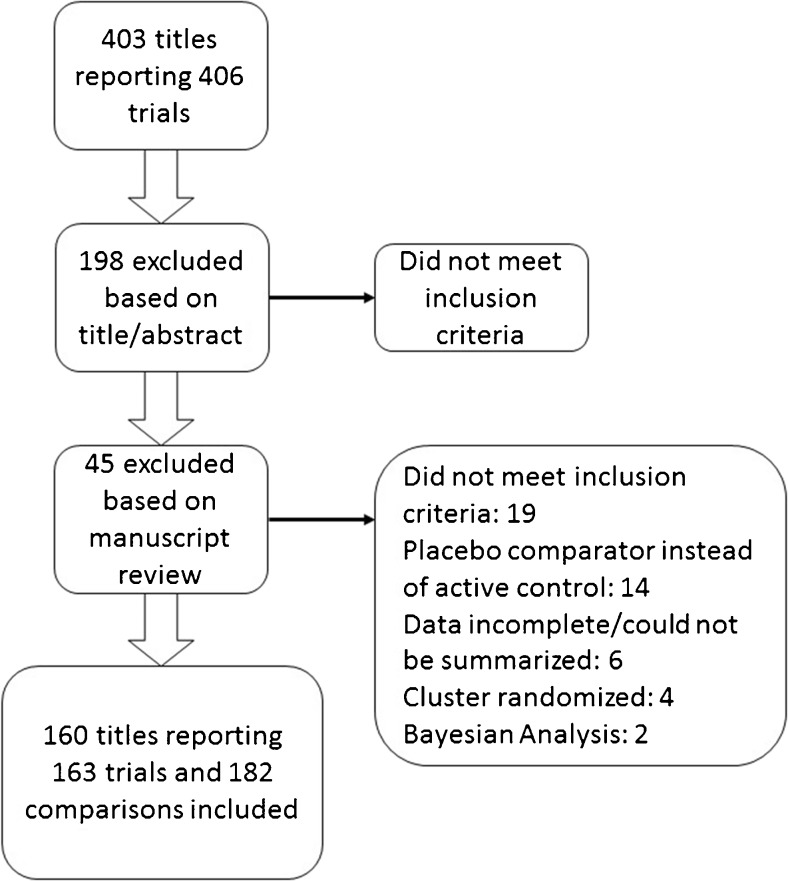
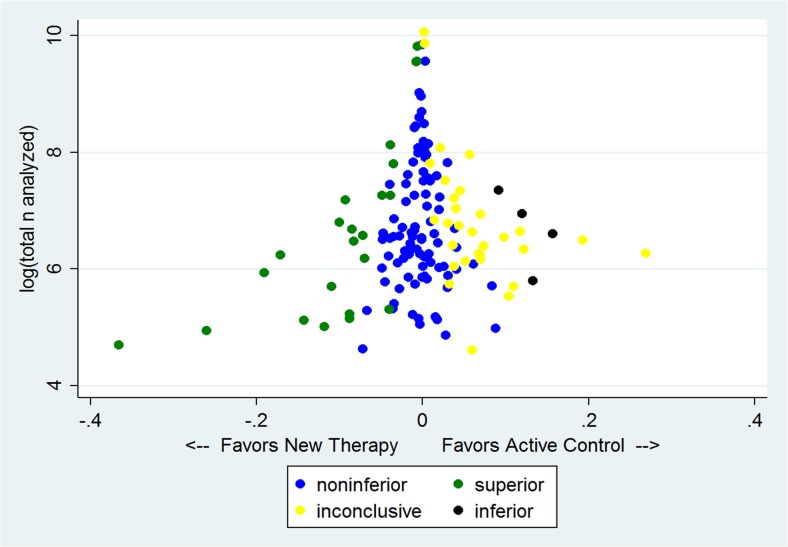
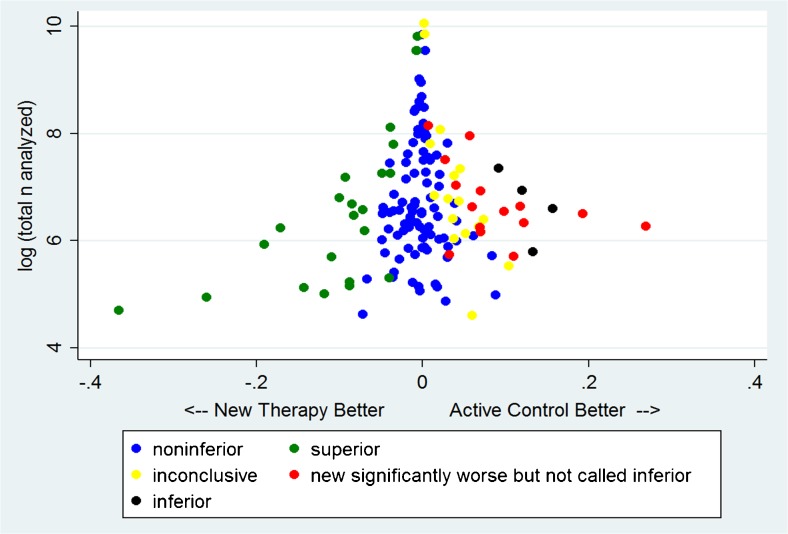
Key results: One hundred sixty-three trials and 182 noninferiority comparisons were included in our analysis. Based on CONSORT-recommended interpretation, 79% of experimental therapies met criteria for noninferiority, 13% met criteria for superiority, 20% were declared inconclusive, and 2% met criteria for inferiority. However, for 12% of trials, the experimental therapy was statistically significantly worse than the active control, but CONSORT recommended an interpretation of inconclusive or noninferior. A two-sided alpha equivalent of greater than 0.05 was used in 34% of the trials, and in five of these trials, the use of a standard two-sided alpha of 0.05 led to changes in the interpretation of results that disfavored the experimental therapy. In four of the five comparisons where different methods of analysis (e.g., intention-to-treat and per-protocol) yielded different results, the intention-to-treat analysis was the more conservative. In 11% of trials, a secondary advantage of the new therapy was neither reported nor could it be inferred by reviewers.
Conclusions: In this cohort, the design and interpretation of noninferiority trials led to significant and systematic bias in favor of the experimental therapy. Clinicians should exercise caution when interpreting these trials. Future trials may be more reliable if design parameters are standardized.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Comment in
-
Non-Inferiority Trials in Medicine: Practice Changing or a Self-Fulfilling Prophecy?J Gen Intern Med. 2018 Jan;33(1):3-5. doi: 10.1007/s11606-017-4191-y. J Gen Intern Med. 2018. PMID: 28980180 Free PMC article. No abstract available.
-
Design and Interpretation of Noninferiority Trials.J Gen Intern Med. 2018 Aug;33(8):1216. doi: 10.1007/s11606-018-4503-x. J Gen Intern Med. 2018. PMID: 29845471 Free PMC article. No abstract available.
-
Design and Interpretation of Noninferiority Trials.J Gen Intern Med. 2018 Aug;33(8):1217. doi: 10.1007/s11606-018-4505-8. J Gen Intern Med. 2018. PMID: 29845472 Free PMC article. No abstract available.
-
Design and Interpretation of Noninferiority Trials.J Gen Intern Med. 2018 Aug;33(8):1215. doi: 10.1007/s11606-018-4504-9. J Gen Intern Med. 2018. PMID: 29948802 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
