

Multiscale technologies for treatment of ischemic cardiomyopathy
- PMID: 28875984
- PMCID: PMC5717755
- DOI: 10.1038/nnano.2017.167
Multiscale technologies for treatment of ischemic cardiomyopathy
Abstract
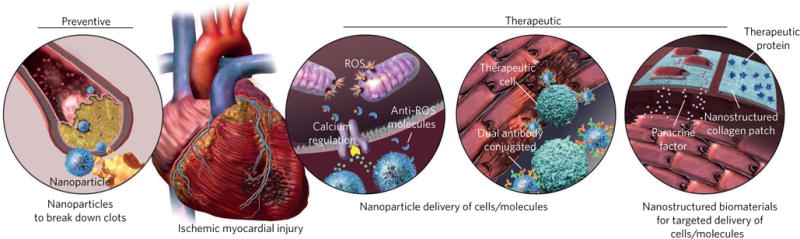
The adult mammalian heart possesses only limited capacity for innate regeneration and the response to severe injury is dominated by the formation of scar tissue. Current therapy to replace damaged cardiac tissue is limited to cardiac transplantation and thus many patients suffer progressive decay in the heart's pumping capacity to the point of heart failure. Nanostructured systems have the potential to revolutionize both preventive and therapeutic approaches for treating cardiovascular disease. Here, we outline recent advancements in nanotechnology that could be exploited to overcome the major obstacles in the prevention of and therapy for heart disease. We also discuss emerging trends in nanotechnology affecting the cardiovascular field that may offer new hope for patients suffering massive heart attacks.
Conflict of interest statement
R.L. and O.C.F. declare financial interests in Selecta Biosciences, Tarveda Therapeutics and Placon Therapeutics. R.L. declares financial interests in Moderna.
Figures
References
-
- Johnson NB, et al. CDC National Health Report: leading causes of morbidity and mortality and associated behavioral risk and protective factors—United States, 2005–2013. MMWR Surveill Summ. 2014;63:3–27. - PubMed
-
- Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50:2173–2195. - PubMed
-
- White HD, Chew DP. Acute myocardial infarction. Lancet. 2008;372:570–584. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
