

Thermodilution vs Estimated Fick Cardiac Output Measurement in Clinical Practice: An Analysis of Mortality From the Veterans Affairs Clinical Assessment, Reporting, and Tracking (VA CART) Program and Vanderbilt University
- PMID: 28877293
- PMCID: PMC5710449
- DOI: 10.1001/jamacardio.2017.2945
Thermodilution vs Estimated Fick Cardiac Output Measurement in Clinical Practice: An Analysis of Mortality From the Veterans Affairs Clinical Assessment, Reporting, and Tracking (VA CART) Program and Vanderbilt University
Abstract
Importance: Thermodilution (Td) and estimated oxygen uptake Fick (eFick) methods are widely used to measure cardiac output (CO). They are often used interchangeably to make critical clinical decisions, yet few studies have compared these approaches as applied in medical practice.
Objectives: To assess agreement between Td and eFick CO and to compare how well these methods predict mortality.
Design, setting, and participants: This investigation was a retrospective cohort study with up to 1 year of follow-up. The study used data from the Veterans Affairs Clinical Assessment, Reporting, and Tracking (VA CART) program. The findings were corroborated in a cohort of patients cared for at Vanderbilt University, an academic referral center. Participants were more than 15 000 adults who underwent right heart catheterization, including 12 232 in the Veterans Affairs cohort between October 1, 2007, and September 30, 2013, and 3391 in the Vanderbilt cohort between January 1, 1998, and December 31, 2014.
Exposures: A single cardiac catheterization was performed on each patient with CO estimated by both Td and eFick methods. Cardiac output was indexed to body surface area (cardiac index [CI]) for all analyses.
Main outcomes and measures: All-cause mortality over 90 days and 1 year after catheterization.
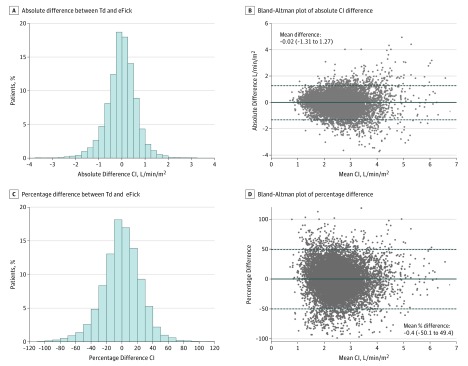
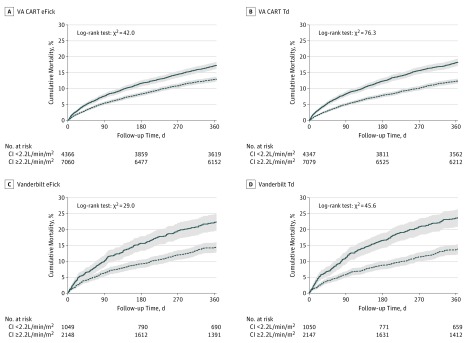
Results: Among 12 232 VA patients (mean [SD] age, 66.4 [9.9] years; 3.3% female) who underwent right heart catheterization in this cohort study, Td and eFick CI estimates correlated modestly (r = 0.65). There was minimal mean difference (eFick minus Td = -0.02 L/min/m2, or -0.4%) but wide 95% limits of agreement between methods (-1.3 to 1.3 L/min/m2, or -50.1% to 49.4%). Estimates differed by greater than 20% for 38.1% of patients. Low Td CI (<2.2 L/min/m2 compared with normal CI of 2.2-4.0 L/min/m2) more strongly predicted mortality than low eFick CI at 90 days (Td hazard ratio [HR], 1.71; 95% CI, 1.47-1.99; χ2 = 49.5 vs eFick HR, 1.42; 95% CI, 1.22-1.64; χ2 = 20.7) and 1 year (Td HR, 1.53; 95% CI, 1.39-1.69; χ2 = 71.5 vs eFick HR, 1.35; 1.22-1.49; χ2 = 35.2). Patients with a normal CI by both methods had 12.3% 1-year mortality. There was no significant additional risk for patients with a normal Td CI but a low eFick CI (12.9%, P = .51), whereas a low Td CI but normal eFick CI was associated with higher mortality (15.4%, P = .001). The results from the Vanderbilt cohort were similar in the context of a more balanced sex distribution (46.6% female).
Conclusions and relevance: There is only modest agreement between Td and eFick CI estimates. Thermodilution CI better predicts mortality and should be favored over eFick in clinical practice.
Conflict of interest statement
Figures

References
-
- Ganz W, Donoso R, Marcus HS, Forrester JS, Swan HJ. A new technique for measurement of cardiac output by thermodilution in man. Am J Cardiol. 1971;27(4):392-396. - PubMed
-
- Dehmer GJ, Firth BG, Hillis LD. Oxygen consumption in adult patients during cardiac catheterization. Clin Cardiol. 1982;5(8):436-440. - PubMed
-
- LaFarge CG, Miettinen OS. The estimation of oxygen consumption. Cardiovasc Res. 1970;4(1):23-30. - PubMed
-
- Bergstra A, van Dijk RB, Hillege HL, Lie KI, Mook GA. Assumed oxygen consumption based on calculation from dye dilution cardiac output: an improved formula. Eur Heart J. 1995;16(5):698-703. - PubMed
-
- Guyton AC, Jones CE, Coleman TG. Cardiac Output and Its Regulation. 2nd ed Philadelphia, PA: Saunders; 1973.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
