

Antibody-associated CNS syndromes without signs of inflammation in the elderly
- PMID: 28878050
- PMCID: PMC5631166
- DOI: 10.1212/WNL.0000000000004541
Antibody-associated CNS syndromes without signs of inflammation in the elderly
Abstract
Objective: To report the CNS syndromes of patients ≥60 years of age with antibodies against neuronal surface antigens but no evidence of brain MRI and CSF inflammatory changes.
Methods: This was a retrospective clinical analysis of patients with antibodies against neuronal surface antigens who fulfilled 3 criteria: age ≥60 years, no inflammatory abnormalities in brain MRI, and no CSF pleocytosis. Antibodies were determined with reported techniques.
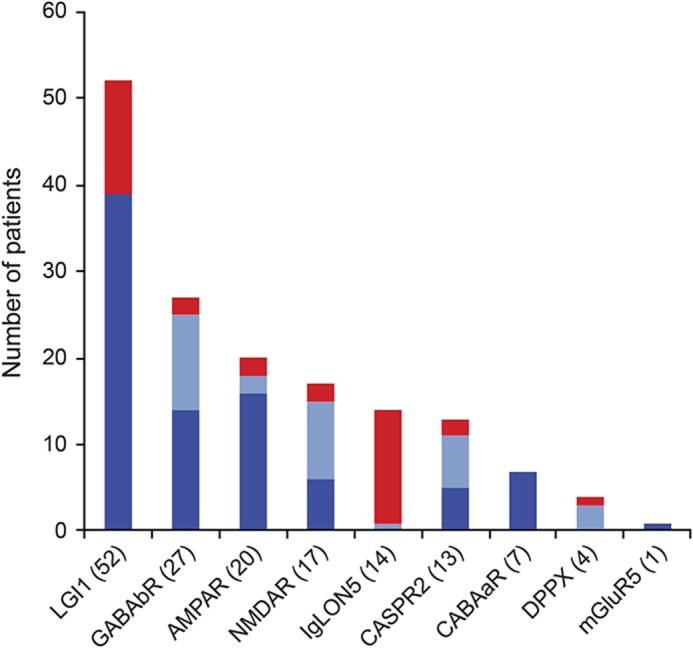
Results: Among 155 patients ≥60 years of age with neurologic syndromes related to antibodies against neuronal surface antigens, 35 (22.6%) fulfilled the indicated criteria. The median age of these 35 patients was 68 years (range 60-88 years). Clinical manifestations included faciobrachial dystonic seizures (FBDS) in 11 of 35 (31.4%) patients, all with LGI1 antibodies; a combination of gait instability, brainstem dysfunction, and sleep disorder associated with IgLON5 antibodies in 10 (28.6%); acute confusion, memory loss, and behavioral changes suggesting autoimmune encephalitis (AE) in 9 (25.7%; 2 patients with AMPAR, 2 with NMDAR, 2 with GABAbR, 2 with LGI1, and 1 with CASPR2 antibodies); and rapidly progressive cognitive deterioration in 5 (14.3%; 3 patients with IgLON5 antibodies, 1 with chorea; 1 with DPPX antibody-associated cerebellar ataxia and arm rigidity; and 1 with CASPR2 antibodies).
Conclusions: In patients ≥60 years of age, the correct identification of characteristic CNS syndromes (FBDS, anti-IgLON5 syndrome, AE) should prompt antibody testing even without evidence of inflammation in MRI and CSF studies. Up to 15% of the patients developed rapidly progressive cognitive deterioration, which further complicated the differential diagnosis with a neurodegenerative disorder.
© 2017 American Academy of Neurology.
Figures
References
-
- Irani SR, Stagg CJ, Schott JM, et al. . Faciobrachial dystonic seizures: the influence of immunotherapy on seizure control and prevention of cognitive impairment in a broadening phenotype. Brain 2013;136:3151–3162. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical